Review of the Institute of Human Development, Child and Youth Health
Report of the IHDCYH Review Panel
December 2020
At the Canadian Institutes of Health Research (CIHR), we know that research has the power to change lives. As Canada's health research investment agency, we collaborate with partners and researchers to support the discoveries and innovations that improve our health and strengthen our health care system.
Canadian Institutes of Health Research
160 Elgin Street, 9th Floor
Address Locator 4809A
Ottawa, Ontario K1A 0W9
This publication was produced by the Canadian Institutes of Health Research. The views expressed herein do not necessarily reflect those of the Canadian Institutes of Health Research.
IHDCYH Review Panel:
Chair: Frank Gavin, CHILD-BRIGHT Citizen Engagement Director; Founder and Director, Canadian Family Advisory Network (CFAN).
Panel Members:
- Meghan Azad, Assistant Professor, Pediatrics & Child Health and Community Health Sciences, University of Manitoba; Research Scientist, Children's Hospital Research Institute of Manitoba.
- Sandra Davidge, Director, Women's and Children's Health Research Institute (WCHRI); Professor, University of Alberta.
- Mark Hanson, Professor, Faculty of Medicine, University of Southampton, UK; Founder member and ex-President of International Society for DOHaD.
- Patrick McGrath, VP Research, Innovation and Knowledge Translation IWK and Nova Scotia Health Authority; Professor, Psychology, Pediatrics and Psychiatry, Dalhousie University.
- Anne Monique Nuyt, Head, Division of Neonatology and Center of Excellence in Neonatology, CHU Sainte-Justine; Professor of Pediatrics, Université de Montréal.
Thanks to all participants in this review and the CIHR IHDCYH Review Team: Ian Raskin, Michael Goodyer, Carmelle Goldberg, Jenny Larkin, Jonathan Gilbert, Daniela Corno, and Emily Guerette.
And special thanks to:
- Shoo K. Lee, Scientific Director, IHDCYH,
- Sarah De La Rue, PhD, Assistant Director, IHDCYH,
- Ruth Warre, PhD, Senior Scientific Associate, IHDCYH and the IHDCYH team.
For more information and to obtain copies, please contact : evaluation@cihr-irsc.gc.ca
Table of Contents
I. Executive Summary
The review of the Institute of Human Development, Child and Youth Health (IHDCYH) was undertaken by the Canadian Institutes of Health Research (CIHR) as part of the rolling reviews of the mandate and performance of CIHR Institutes initiated by CIHR's Governing Council (GC) in 2015 and mandated by the CIHR Act. The review assessed the relevance and performance of IHDCYH from 2000 to 2018, with a focus on 2012 to 2018, to inform the future direction and focus of its mandate, and meet the requirements of the CIHR Act and the Policy on Results. The review was conducted by the CIHR Evaluation Unit and overseen by a panel of experts in IHDCYH's mandate areas, the IHDCYH Review Panel (hereafter referred to as the Panel), who reviewed and interpreted the findings and made the final recommendations. The recommendations and observations of the Panel are summarized below in relation to the two broad issues addressed by the review.
A. Are changes needed within the current IHDCYH mandate in order to address emerging areas of research?
IHDCYH has advanced knowledge and built capacity in mature fields of research, maintained investments in niche areas of research, and invested in emerging areas in its mandate. The Panel commends IHDCYH's progress in skillfully bringing together Institutes and international partners for the Healthy Life Trajectories Initiative (HeLTI), its leadership and collaborating role in eleven CIHR Initiatives, and its stewardship of continuing negotiations for a streamlined National Ethics Review Board or process—to name a few highlights under Dr. Lee's tenure as Scientific Director (SD).
The Panel cautions against a dramatic shift in current priorities but encourages the updating of priorities to address unmet needs and areas of emerging research. IHDCYH's mandate would benefit from an update that reflects the shift in paradigm towards a life-cycle—as distinct from a life-course—approach and an emphasis on prevention, including the integration of parental health and the underlying psychosocial as well as biological causes of disease. Based on extensive Panel discussion, for purposes of this report, the life-cycle approach is regarded as both linear (considering the health of the embryo, the fetus, the infant, the child, adolescent, and adult) and cyclical (considering the effects of the health of a parent-to-be on the health not only of the yet-to-be-born but of the yet-to-be-conceived).
The Panel expects the proposed modifications will encourage partnerships with key stakeholder groups such as the Maternal Infant Child Youth Research Network (MICYRN). It would also enhance research in the areas identified by key informants, including the health of Indigenous children and families, the social determinants of health, precision medicine, parental health and environmental health.
The panel sees several gaps, emerging areas and new opportunities with IHDCYH's mandate that need to be considered by the Institute going forward. Building on CIHR's Action Plan: Building a healthier future for First Nations, Inuit, and Métis Peoples and partnering with the Institute of Indigenous Peoples Health (IIPH), it will be important for IHDCYH to invest in research which increases capacity of Indigenous communities to conduct research. The Panel further agrees on the importance of enhancing research and partnerships to address current gaps (e.g., adolescent health, precision medicine) and harness big data (especially from cohort studies, genomics and other "-omics" such as proteomics, metabolomics, microbiomics, epigenomics), artificial intelligence, regenerative medicine, clinical, social, and other records, as well as new drugs and devices. The Panel also concludes that there should be more opportunities for, and a greater receptivity to, mixed-methods and qualitative research given the interdisciplinary nature of research within its mandate.
The Panel is concerned that there may be a limited pool of investigators in the research pipeline to replace senior investigators and significant disincentives for clinical investigators to be involved in research due to a number of factors including low funding rates and modes of remuneration. There was consensus among Panel members that IHDCYH should work in collaboration with CIHR and relevant associations to inform and support the implementation of CIHR's Strategic Action Plan on Training and look to leverage existing training and career support programs such as the Canadian Child Health Clinician Scientist Program (CCHCSP).
The Panel regards an increased focus on succession planning in IHDCYH investments as essential moving forward. For example, the Panel identified the need for continued investments in improving trial designs for team grants that includes practicing clinicians, social scientists, and investigators at all career stages.
Recommendation 1: The Panel recommends that Governing Council review the current mandate and consider integrating a life-cycle approach thereby embracing and contributing to a paradigm shift in the scientific landscape. This would include an emphasis on parental and not just maternal health and on the psychosocial and biological causes of disease.
Recommendation 2: The Panel recommends that IHDCYH engage its broad researcher and stakeholder communities to identify ways to address current research gaps and emerging areas of research and to apply novel research approaches as well as new and developing tools.
Recommendation 3: The Panel recommends that IHDCYH enhance partnerships related to the health of Indigenous children and families to increase capacity especially focused on Indigenous researchers and communities.
Recommendation 4: The Panel recommends that IHDCYH and CIHR develop a predictable and sustainable funding pipeline across all career stages by continuing to embed capacity-building activities in all of its funding opportunities. Specifically, this would entail including financial, mentorship, and training components in capacity-building activities and leveraging other capacity-building programs.
Recommendation 5: The Panel recommends that CIHR, in collaboration with Institutes, address the challenges associated with the peer review of interdisciplinary research across CIHR's four research themes and of emerging and high-risk areas of research.
Recommendation 6: The Panel recommends that IHDCYH continue to build capacity to develop innovative ways to translate knowledge to clinicians, policy makers, organizations, and the public in order to develop more effective therapeutics, practices, policies and services to improve the health of Canadians and the health care system.
B. Observations and Recommendations for the Next Scientific Director
The Panel recognizes that the current SD's strong ability to engage, collaborate, and partner with a wide range of stakeholders at the national and international levels has fostered many successful partnerships under IHDCYH's mandate. This was true even during times of unprecedented change and resource constraints at CIHR. The limited available financial resources in the Institute's research budget will require the next SD to be both innovative and persistent in carrying out his or her convener and catalyst roles to help researchers identify potential partners and opportunities as they make their way through the landscape of life-cycle research as well as engage and leverage other national cohorts such as the Canadian Healthy Infant Longitudinal Development (CHILD) Study and the Maternal-Infant Research on Environmental Chemicals (MIREC) Study. The Panel sees the convening and influencing roles as being as important as the funding role. Moreover, it will be important for the next SD to build on, rather than abandon or simply allow to proceed, the work of the previous SD.
Recommendation 7: The Panel recommends that IHDCYH's next SD continue to work hard to mainstream the life-cycle concept and to highlight and embed the importance of children and parents within CIHR and its Institutes and, more broadly, with its national and international research partners and stakeholder communities.
Recommendation 8: The Panel recommends that IHDCYH's SD continue to work collaboratively with CIHR to build awareness of large national and international platforms like HeLTI, leverage partnerships that help sustain and promote the use of such platforms, and engage with other national cohorts, pediatric trial networks, biobanks, and databases.
Recommendation 9: The Panel recommends that IHDCYH incorporate sustainability planning at the time of the design of funding opportunities (e.g., phase two funding, wind-down or knowledge translation funding) to provide more predictable and sustainable funding mechanisms, and monitor key performance measures related to the impacts of funding opportunities.
II. Overview of the Review
A. Review Objectives
The review of the Institute of Human Development, Child and Youth Health (IHDCYH) is part of the rolling review of the mandate and performance of CIHR Institutes initiated by CIHR's Governing Council (GC) in 2015. The review assesses the relevance and performance of IHDCYH to inform future direction and focus of its mandate, and meet the requirements of the CIHR Act and the Policy on Results. The aim of the review is to provide CIHR's Senior Leadership Committee and Governing Council with valid and reliable findings to inform decisions related to:
- Whether changes are needed within the current IHDCYH mandate to address emerging areas of research; and
- The transition of the Institute to the next Scientific Director.
The review is overseen by the IHDCYH Review Panel, comprised of experts in the IHDCYH mandate areas, who will review and interpret the findings and make final recommendations. The names and affiliations of the Panel members are listed in Appendix 1.The review includes the period of 2000-01 to 2018-19, with a specific focus on the period under the leadership of the current SD, Dr. Shoo K. Lee, from 2012 to 2019. The review draws on multiple lines of evidence, including qualitative and quantitative data sources.
B. CIHR Context
As outlined in the CIHR Act, the objective of the CIHR is:
“to excel, according to internationally accepted standards of scientific excellence, in the creation of new knowledge and its translation into improved health for Canadians, more effective health services and products and a strengthened Canadian health care system…”
Among the many activities to achieve its objective, CIHR is responsible for:
- promoting the dissemination of knowledge and the application of health research to improve the health of Canadians;
- encouraging innovation, facilitating the commercialization of health research in Canada and promoting economic development through health research in Canada; and,
- building the capacity of the Canadian health research community through the development of researchers and the provision of sustained support for scientific careers in health research.
As divisions within CIHR, the Institutes are expected to encourage interdisciplinary, integrative health research and contribute to the achievement of CIHR's overall objective within their mandate. The Institutes are to: pertain to all aspects of health; include research across all four research themes; work in collaboration with the provinces to advance health research and to promote the dissemination and application of new research knowledge to improve health and health services; and, engage voluntary organizations, the private sector and others, in or outside Canada, with complementary research interests.
In terms of funding, the Government of Canada has made significant investments in research and innovation in Budget 2018. For CIHR, this translates to an investment of $354.7M phased in over 5 years and $90.1M ongoing in CIHR's Investigator-Initiated Research program budgetFootnote 1. The Budget increase follows the final report of the Government of Canada's Review of Federal Support for Fundamental Science, released on April 10, 2017, which stressed the need for significant reinvestment in the federal research ecosystem over a more predictable and better planned multi-year horizon, as well as improved coordination and collaborations between the three federal granting agencies (CIHR, Natural Sciences and Engineering Research Council of Canada [NSERC], and Social Sciences and Humanities Research Council of Canada [SSHRC]) and the Canada Foundation for Innovation (CFI)Footnote 2. Prior to Budget 2018, CIHR's budget had been effectively flat for approximately the last 10 years, and therefore it was declining substantially in real terms, greatly affecting the ability of researchers to sustain competitive research programs. CIHR funding of research under the 13 Institute mandates is dominated by CIHR investments in the investigator-initiated operating grant competition compared to the priority-driven grants and awards. The Institute's budgets are part of the Research in Priority Areas program budget, which enable Institutes to play a catalyst role with strategically placed investments.
CIHR is composed of 13 virtual Institutes. The original slate of Institutes was designed to ensure not only representation of all sectors and "themes" of health research, but also to provide a home base for each health researcher in CanadaFootnote 3. Each Institute received a strategic research budget of $8.6M until 2014-15. As a result of the Institute Modernization, in 2015-16, half of each Institutes' strategic research budgets ($4.3 M per year) was invested in CIHR's Roadmap Accelerator Fund (RAF) to support multi-Institute and multidisciplinary initiatives that aligned with CIHR's research priorities and were patterned along the lines of existing CIHR Initiatives. The remaining half of the budget remains under the control of Institutes to direct toward Institute-specific initiatives. The RAF process was perceived by Institutes as limiting the ability of the Institutes to invest their strategic funds in Institute-specific priority areas. As of 2017-18, the RAF ended and starting in 2018-19, unplanned RAF funding was redistributed to the Institutes to progressively increase their budget to $8.6M (reached in 2027-28). Moving forward, the investments of funds in multi-Institute and multidisciplinary initiatives are guided by the same "spirit" and principles as RAF.
III. Observations and Recommendations
A. Are changes needed within the current IHDCYH mandate to address emerging areas of research?
1. Panel Observations
The Panel acknowledges that IHDCYH is a unique institute within CIHR as it is focused on the life trajectory from prenatal life to adulthood and encompasses CIHR's four research themes: biomedical, clinical, health systems and services, and social, cultural, environmental, and population health. IHDCYH has a broad mandate and a limited budget to support research within an extremely diverse research and stakeholder community with very different needs. To date, IHDCYH has worked to advance and translate knowledge, build research capacity and have an impact within its three investment themes and six strategic priorities. At this point, the Panel observes that a substantial shift in direction and priorities would be detrimental given its hard-won and significant achievements. That said, the Panel concludes that IHDCYH's mandate would benefit from an update that reflects the shift in paradigm towards a life-cycle approach and an emphasis on prevention, including the integration of parental health and the underlying psychosocial and biological causes of disease.
The Panel agrees that the proposed modifications may enhance research and partnerships on the unmet needs identified by key informants, including research on the social determinants of health, policy-driven research, and patient-oriented research as well as research related to adolescent health, precision medicine, parental health, positive health and well-being, and environmental health. The Panel further agrees on the importance of enhancing research and partnerships to harness big data, especially from cohort studies, genomics, proteomics and metabolomics, artificial intelligence, regenerative medicine, clinical, social and other records, as well as new drugs and devices.
The Panel notes the achievements of IHDCYH in terms of international leadership and legacy within the Developmental Origins of Health and Disease through the Lifespan (DOHaD) strategic priority through HeLTI. However, the Panel stresses the importance of other research priorities with IHDCYH's limited budget. As such, the Panel sees the importance for health research to help reduce health inequities that currently exist in Canada, most notably but not only between Indigenous and non-Indigenous people. This should include supporting research by and with Indigenous communities and increasing the capacity of Indigenous communities to conduct research and partner with the broader research community. To be successful, this will require an openness to grassroots approaches and partnership with CIHR's Institute of Indigenous Peoples' Health (IIPH) to support for Indigenous research in parental and child health.
In terms of both IHDCYH's interdisciplinary mandate and additional partnerships within CIHR, the Panel observes the need to increase awareness of how CIHR supports interdisciplinary and social science research and improve peer review culture and expertise to better ensure fair and transparent assessments of interdisciplinary research projects. The Panel and key informants observed the need for greater opportunity and receptivity towards social science, mixed-methods and qualitative research to ensure that interdisciplinary approaches are valued as often necessary to address complex child and parental health issues. To address this issue, IHDCYH will need to collaborate with CIHR's Vice-President, Research Programs and key branches within the Research Programs Portfolio such as the Program Design and Delivery Branch, responsible for competition design and delivery, and the Science Policy Branch, responsible for the College of Reviewers and Science Strategy teams.
Panel members and key informants observe that there is a limited pool of investigators to replace senior investigators in the research pipeline and significant disincentives for clinical investigators to be involved in research due to a number of factors including low funding rates and modes of remuneration. There was consensus among panel members that IHDCYH should work in collaboration with CIHR and relevant associations to inform and support the implementation of CIHR's Strategic Action Plan on Training, including leveraging existing programs like the Canadian Child Health Clinician Scientist Program (CCHCSP) which may need to expand its focus to include trainees. It will be important when planning capacity-building investments to identify the area or career path being targeted: needs (financial, training, mentorship), research area/theme, or career stage or path as researchers' transition from early-career to mid-career to senior researchers. In case of research initiatives with embedded capacity building, it will important to have meaningful indicators of impact on participants.
2. Recommendations
Recommendation 1: The Panel recommends that Governing Council review the current mandate and consider integrating a life-cycle approach thereby embracing and contributing to a paradigm shift in the scientific landscape. This would include an emphasis on parental and not just maternal health and on the psychosocial and biological causes of disease.
Recommendation 2: The Panel recommends that IHDCYH engage its broad researcher and stakeholder communities to identify ways to address current research gaps, emerging areas of research, and novel research approaches as well as new and developing tools.
Recommendation 3: The Panel recommends that IHDCYH enhance partnerships related to the health of Indigenous children and families to increase capacity especially focused on Indigenous researchers and communities.
Recommendation 4: The Panel recommends that IHDCYH and CIHR develop a predictable and sustainable funding pipeline across all career stages by continuing to embed capacity-building activities in all of its funding opportunities. Specifically, this would include financial, mentorship, and training components in capacity-building activities and leveraging other capacity building programs.
Recommendation 5: The Panel recommends that CIHR, in collaboration with Institutes, address the challenges associated with the peer review of interdisciplinary research across CIHR's four research themes, and emerging and high-risk areas of research.
Recommendation 6: The Panel recommends that IHDCYH continue to build capacity to develop innovative ways to translate knowledge to clinicians, policy makers, organizations, and the public in order to develop more effective therapeutics, practices, policies and services to improve the health of Canadians and the health care system.
B. Observations for the Next Scientific Director
1. Panel Observations
The Panel recognizes that the current SD's strong ability to engage, collaborate, and partner with a wide range of stakeholders at the national and international levels has fostered many successful partnerships under IHDCYH's mandate. This was true even during times of unprecedented change and fiscal constraint. The limited available financial resources in the Institute's research budget will require innovation in convener and catalyst roles to help researchers navigate partner and researcher landscapes with respect to life-cycle research. The Panel sees the convening and influencing roles of the SD as being just as important as the funding role.
The Panel commends Dr. Lee and the Institute for the accumulated surplus to support Institute operations during the transition period to the next SD. The Panel observes that IHDCYH has incurred a higher than anticipated workload and has had to increase the number of host institution staff with the same operational budget since the move from Ottawa-based Institute staff (OBIS) to Integrated Institute Teams (IIT) at CIHR. It will be important for CIHR, as part of the Institute Support Optimization Project, to consider the importance of consistent and dedicated CIHR staff in supporting and enhancing an SD and the Institute's ability to convene and influence with other Institutes, CIHR, Canadian stakeholders, and international organizations.
An important area for the next SD and Institute should be to advocate for the life-cycle approach and child health research within CIHR and with other Institutes to build awareness of the importance of, and increase support for more investment in the areas of IHDCYH's mandate. Simply put, child health research is not solely within the purview of IHDCYH but needs to be integrated into other Institutes' initiatives and funding opportunities. For example, the new SD could make the case inside and outside CIHR that in an aging society the health and well-being of children and youth are ever more important in relation to social stability, societal health, and economic prosperity. Beyond CIHR, it will be important to build on the work and achievements of the Institute to enhance awareness and foster support internationally.
Related to, yet distinct from mainstreaming of the life-cycle approach, the Panel feels it is imperative that IHDCYH and CIHR continue to invest in HeLTI to sustain the momentum, expand partnerships, and maximize the exploitation of the platform. HeLTI has been a very successful intervention research initiative that has helped to establish Canada as a world leader in Developmental Origins of Health and Disease (DOHaD) research and will yield an extraordinarily valuable and unique dataset and biobank based on the four harmonized cohorts that will provide key results related to important connections between non-communicable diseases (NCDs) and preconception with real potential to impact global health. Going forward, it will be important for IHDCYH and CIHR to: retain the vision to protect and open the dataset to a broad range of scientists; sustain funding from CIHR and current partners for the platform; engage other funders and cohorts (e.g., South America); and launch funding mechanisms to facilitate the use of the resource to develop both careers and knowledge.
The Panel commends Dr. Lee and IHDCYH's work in skillfully bringing together Institutes and international partners for HeLTI, its leadership and collaborating role in eleven CIHR Initiatives; and the stewardship of continuing negotiations for a future streamlined national Ethics Review Board (REB) approvals (e.g. Pediatric REB Initiative). In order to further strengthen Canadian health research and position Canada as a global leader in research, the Panel agrees IHDCYH will need to establish more presence, and engage with national and international partners and potential partners. The Panel suggests that IHDCYH actively consider partnerships and collaborations with Children's Healthcare Canada (formerly CAPHC), the Maternal, Infant, Child, and Youth Research Network (MICYRN), and the Canadian Institute for Advanced Research (CIFAR), especially its Child and Brain Development Program. In terms of international partnerships, key informants suggested partnerships with international non-government organizations including: Wellcome Trust; Bill and Melinda Gates Foundation; National Institutes of Health (NIH), notably, the National Institute of Child Health and Human Development (NICHD); European clinical trial groups; charities, philanthropies, and civil society groups; professional groups; and pediatric trials networks such as the Pediatric Trials Network (PTN) in the US.
The Panel noted that there is a need for an increased focus on succession planning of IHDCYH investments, especially larger investments such as team grants, at the outset to provide predictable funding pipelines to shepherd and sustain the initiative and/or capture and translate the knowledge created. Related to this, there is a need to provide information and guidance to current grant holders about the nature and timing of potential additional and related funding, and also assist with partnerships. This should include continued investments in improving trial design through team grants that include practicing clinicians, social scientists, methodologists, investigators at all career stages, and end-user stakeholders (e.g. policy makers and trial researchers). Similarly, looking to include intervention components in research through natural experiments, prevention trials, and pilot studies to bridge the gap between fundamental research and applied research were observed as promising paths forward.
2. Recommendations
Recommendation 7: The Panel recommends that IHDCYH's next SD continue to work hard to mainstream the life-cycle concept and to highlight and embed the importance of children and parents within CIHR and its Institutes and, more broadly, with its national and international research partners and stakeholder communities.
Recommendation 8: The Panel recommends that IHDCYH's SD continue to work collaboratively with CIHR to build awareness of large national and international platforms like HeLTI, leverage partnerships that help sustain and promote the use of such platforms, and engage with other national cohorts, pediatric trial networks, biobanks, and databases.
Recommendation 9: The Panel recommends that IHDCYH incorporate sustainability planning at the time of the design of funding opportunities (e.g. phase two funding, wind-down or knowledge translation funding) to provide more predictable and sustainable funding mechanisms, and monitor key performance measures related to the impacts of funding opportunities.
IV. Key Findings
A. Relevance
1. Ongoing relevance of the IHDCYH mandate
IHDCYH's mandate is to support research to enhance maternal, child, and youth health and to address causes, prevention, screening, diagnosis, treatment, short- and long-term support needs, and palliation for a wide range of health concerns associated with reproduction, early development, childhood, and adolescence. IHDCYH embraced the findings from the 2011 International Review and suggestions from more than 1,000 members of IHDCYH's community through an environmental scan, in-person consultations, web survey, key informant interviews, focus groups, and a strategic planning retreat. Moving forward under the direction of Dr. Lee, IHDCYH's 2013-17 Strategic Plan: Healthy Foundations of Life offered a new approach to supporting excellence in the development of new knowledge. To realize IHDCYH's mandate, the Institute has taken a life course approach, with both the 2013-17 Strategic Plan and 2018-20 Refreshed Strategic Plan focused on three overarching research investment themes, each with two strategic priorities:
- 1. Healthy Developmental Trajectories:
- 1.1 Developmental Origins of Health and Disease through the Lifespan (DOHaD) is a multi-disciplinary field that examines how environmental factors acting during the phase of developmental plasticity interact with genotypic variation to change the capacity of the individual to cope with its environment.
- 1.2 Preterm Birth focuses on identifying Canadian priorities within the global context, including prevention, management of at risk pregnancies, and optimization of outcomes both during the perinatal period and on into childhood and beyond.
- 2. Healthy Reproduction, Pregnancy, Childhood and Youth:
- 2.1 Environmental Health aims to increase understanding of the influence of social, physiological and physical elements on reproduction and the growth and development of the embryo, fetus, child, and youth.
- 2.2 Healthy Pregnancy spans research into fertility and infertility, maternal health prior to and during pregnancy, as well as healthy birth and causes of infant mortality.
- 3. Healthy Public Policy and Systems Integration:
- 3.1 Integrated Child and Youth Research and Health Services supports research investments related to: (a) vertical integration of health services from primary through secondary and tertiary level care, as well as health systems administration and policy; (b) horizontal integration of research evidence into initiatives aimed at improving health systems and clinical services; and (c) the integration of the research (both basic and clinical) and clinical enterprises in the health care system.
- 3.2 Mental Health focuses on increasing knowledge about and access to effective mental health prevention interventions for children and youth at risk, other early interventions including early diagnostic services, and effective treatment services for children and youth with established disorders.
These research investments are linked by enabling tactics to strengthen the overall approach: enhancing research capacity; developing partnerships; facilitating knowledge translation; facilitating data sharing; and embracing global health.
The broad, relevant, and well-established scientific enterprise directly associated with IHDCYH's mandate is demonstrated by 1,122,687 publications worldwide between 2000 and 2017 (Figure 1, Appendix 3). While Canada produces only 6% of the world's share of publications in IHDCYH's mandate, it is a leader in informing research agendas worldwide as demonstrated by its ranking of 3rd among top producing countries in terms of Average of Relative Citations and 4th in terms of Average Relative Impact Factor in the broad mandate area (Figure 2-5, Appendix 3). Publications aligned to Healthy Pregnancy represent a mature field of research. Publications aligned to Mental Health, Integrated Child and Youth Research and Health Services, and Preterm Birth were suggestive of niche areas of knowledge production. Publications aligned to Developmental Origins of Health and Disease through the Lifespan and Environmental Health were suggestive of emergent areas of knowledge production.
IHDCYH's work addresses the continued global need to ensure a healthy start to life and promote well-being at all ages, as well as to prevent early indicators of later-life non-communicable diseases in line with United Nations Sustainable Development Goals. At the federal government level, there is continued inter-ministerial support from the Ministers of Health, Indigenous Services, and Families, Children, and Social Development to prioritize research on human development, child and youth health. Within CIHR, IHDCYH's work contributes significantly to the achievement of CIHR objectives by leading or collaborating on 11 CIHR Initiatives aligned with CIHR's strategic priorities. IHDCYH takes a leadership role on CIHR's Healthy Life Trajectories Initiative (HeLTI), the Integrated Cannabis Research Strategy, and Transitions in Care (TiC) while collaborating on eight Major Initiatives described in Figure 6 of Appendix 3. IHDCYH is among the top institute collaborators on CIHR Initiatives.
Significant increases in CIHR investments were aligned to IHDCYH's mandate under Dr. Lee's tenure, suggesting that researchers working in IHDCYH's mandate have been increasingly successful in the investigator-initiated funding programs. Over the first decade and a half of CIHR's operation, IHDCYH consistently ranked 7th or 8th in terms of funding among the thirteen institutes (Figure 7, Appendix 3). Between 2014-15 and 2017-18, IHDCYH's ranking rose to 5th or 6th among the thirteen institutes. Overall, IHDCYH mandate investments are multidisciplinary, integrating health research across all four CIHR themes rather than research in single themes. Approximately 40% of CIHR IHDCYH mandate investments were directed to Biomedical research, 25% were directed to Clinical research, 17% were directed to Social, Cultural, Environmental, and Population Health research respectively, and 7% were directed to Health Systems and Services research (Figure 8, Appendix 3). Approximately 11% of the data for IHDCYH CIHR theme investments are classified as not applicable/specified, demonstrating a challenge to classify the interdisciplinary research, as well as the fact that the themes are self-reported by researchers.
CIHR investment in IHDCYH's strategic priorities remained relatively stable in Developmental Origins of Health and Disease in the Lifespan and Preterm Birth strategic priorities, with these priorities receiving an average of $36M and $20M per year respectively (Figure 9, Appendix 3). Between 2014-15 and 2017-18, there have been continuous increases in investment in the Environmental Health strategic priority ($13.5M in 2014-15 to $45.2M in 2017-18), Healthy Pregnancy strategic priority ($9.7M in 2014-15 to $39.8M in 2017-18), Integrated Child and Youth Research and Health Services strategic priority ($12.4M in 2014-15 to $41.6M in 2017-18), and Mental Health strategic priority ($12.7M in 2014-15 to $53.6M in 2017-18).
Like each of CIHR's 13 institutes, IHDCYH receives a strategic research budget, which following the CIHR Institute Modernization Process in 2015-16, is referred to as the Institute-Specific Initiative (ISI). Between 2002-03 and 2011-12, IHDCYH's budget had an overall increasing trend ranging from $3.8M to $9.7M (Figure 10, Appendix 3)Footnote 4. The budget then remained at the level of $8.6M, which included a top up of $100K for Institute Community Support programs through until 2013-14.
During 2013-14 CIHR introduced an Investment Planning initiative that reallocated funding from Institutes to address corporate strategic investment priorities in years 2014-15 and 2015-16. After this period, as part of the CIHR Institute Modernization process, the ISI was halved from $8.6M to $4.3M, although IHDCYH received some top up to this amount to partially compensate for the monies previously removed. At the same time, CIHR's Roadmap Accelerator Fund (RAF) was introduced to pool the remaining portion of Institute's ISI to support multi-institute and multidisciplinary initiatives aligned with research priorities outlined in CIHR's Roadmap II and selected by the President and Science Council. These two actions resulted in IHDCYH's budget decreasing from $7.8M in 2014-15 to $2.5M in 2015-16. The RAF was in place until 2017-18, at which time the funds were returned to the control of each institute, although still required to be allocated to support RAF initiatives. However, IHDCYH funding commitments to RAF initiatives approved during the period of pooling in 2015-16 and 2016-17 have continued to limit future ISI budget totals. It should be highlighted that due to financial constraints from ongoing commitments from the previous leadership in 2012-13 and 2013-14, and the impacts of the Investment Planning and RAF initiatives, Dr. Lee did not have access to a full ISI budget of $8.6M per year during his tenure as SD, which required the Institute to take a skillful and judicious approach to investment.
Key informants as well as the Panel identified a need to embrace a paradigm shift in the scientific landscape by considering life-cycle; parental as opposed to maternal health; and psychosocial, and biological causes of disease regarding IHDCYH's mandate. Additionally, there is an agreed upon importance to enhance research and partnerships by: harnessing big data from cohort studies, genomics and other "-omics" such as proteomics, metabolomics, microbiomics, epigenomics; clinical, social and other records; new drugs and other therapies; artificial intelligence; and address unmet needs (e.g. research with Indigenous communities, research on the social determinants of health and health inequalities, positive health and well-being, policy-driven research, patient-oriented research, precision medicine, parental health, environmental health, mix-method research, and qualitative research). Two consistent challenges were identified by key informants: 1) IHDCYH's ability to connect and collaborate with Indigenous communities, suggesting the need for additional work to collaborate with IIPH; 2) the need for fair and transparent peer review panels to assess interdisciplinary projects.
B. Impact
1. Knowledge Advancement and Translation Activities
Over the past eight years, IHDCYH has targeted research to advance and translate knowledge that ensures the best outcomes for children, youth, and families. IHDCYH has led or collaborated on 98 funding opportunities that have funded over 581 grants in maternal, reproductive, child and youth health for a total of $168.24M committed over the terms of those grants. This funding includes a significant proportion of funds leveraged from sources other than IHDCYH’s strategic budget, highlighting the importance of research in maternal, reproductive, child and youth health, as well as IHDCYH’s strengths in building strong collaborative relationships with other funding partners.
IHDCYH-led initiatives, such as the Healthy Life Trajectories Initiative (HeLTI), are linking the building of capacity with the creation of knowledge across CIHR's themes, and the translation of this knowledge into public policy in Canada and globally, for the improvement of health. IHDCYH also supported researchers to translate research evidence into improved health research, services, policies, and systems through innovative knowledge translation approaches, such as embedded knowledge translation (KT) strategies, and supporting networking and collaboration opportunities for each initiative, including workshops, forums and platforms that engage with key stakeholders.
Under the Healthy Developmental Trajectories research theme, research investments to address Developmental Origins of Health and Disease through the Lifespan strategic priority are funded through HeLTI and focused on generating the evidence needed to inform national policies and programs that will have a potential to improve health and control non-communicable diseases (NCDs). The improvements to national policies and programs of non-communicable diseases will be informed by four linked international intervention cohorts across multiple countries (South Africa, China, India, and Canada) that are developing interventions (e.g. nutrition, parental social support and mental health, hygiene and infection prevention, and obesity prevention) from preconception through the postnatal period into early childhood. HeLTI activities include several components:
- Five Canadian DOHaD Research Teams ($1.5M each / 5 years) are conducting discovery research, as well as building Canadian capacity within the DOHaD field;
- Three Linked International Intervention Cohorts (HeLTI LIICs) have been established, one in each of South Africa, China and India ($2.5M each / 5 years, matched 1:1 by international partners). This activity has established a unique research collaboration with the World Health Organization (WHO), the National Natural Science Foundation of China, the Department of Biotechnology of India, and the Medical Research Council of South Africa. Each cohort has joint Canadian and location-specific leadership and will conduct interventional research focused on risk-factors for NCDs;
- A Canadian cohort has been established and is aligned with the international cohorts ($15.0M / 10 years); and
- The Canadian DOHaD Cohort Registry, also known as the Research Advancement through Cohort Cataloguing and Harmonization (ReACH) initiative ($1.3M / 5 years), is acting as an enabling platform to HeLTI.
Led by Dr. Isabel Fortier in collaboration with Drs. Stephanie Atkinson, Alan Bocking and William Fraser, ReACH is an enabling platform for HeLTI that has developed a database of metadata and definitions of variables from all relevant longitudinal Canadian DOHaD cohorts, thereby linking them in a way that facilitates larger and better powered studies. ReACH also provides a harmonization platform, data analysis tools, open source software and technical support. Funded by 11 of the 13 CIHR institutes in 2016, ReACH brings together 53 investigators from different fields; contains metadata from 25 Canadian pregnancy and birth cohorts; involves a total of 53,300 mother-child pairs and 17,800 fathers; and provides information on 17 areas, 132 categories and more than 95,500 variables
Within the Preterm Birth strategic priority, IHDCYH launched the Preterm Birth Initiative, which funded six catalyst grants ($200,000 each / 2 years) in 2016 to generate new and innovative ideas in preterm birth research. A range of projects were funded, from prevention/prediction of preterm birth, through approaches to improving care, to developmental follow-up of the Family Integrated Care intervention in the NICU. All the projects are currently ongoing, have peer-reviewed articles either published or in preparation, and are using their findings to support applications for further grant funding following the end of the grants term. For example, one Preterm Birth Catalyst Grantee, Dr. Graeme Smith, has been looking at how to raise the body's production of carbon monoxide (CO) as a means of preventing or treating pre-eclampsia. He has completed some exploratory studies in animal models that have identified potential dietary supplements that increase CO production and could one day be used for therapeutic intervention in pre-eclampsia. The initiative also provided funding for the Preterm Birth Network ($4.25M / 5 years in 2016) and the Perinatal Health Care System Improvement team ($1.15M / 5 years in 2017).
Under the Healthy Reproduction, Pregnancy, Childhood and Youth Research Theme, the investments directed towards the Environmental Health strategic priority have been through two CIHR multi-institute initiatives - the Environments and Health Signature Initiative (EHSI) and the Canadian Epigenetics, Environment and Health Research Consortium (CEEHRC). Within the EHSI funding opportunities, the successful team in the Environmental Urban Health Research Consortium ($4.165M / 5 years) – CANUE (Canadian Urban Environmental Health Research Consortium) – is furthering our understanding on how to design and modify cities to improve, not degrade, population health. CANUE is working to link standardized environmental exposure data about air quality, green spaces, walkability, noise and other aspects of the urban/suburban environment to existing human health data platforms, including incorporating cohorts focusing on reproductive, fetal and/or child health as priority research area. At the mid-point of their grant, CANUE has over 170 members across 13 research teams; completed 50 data requests since October 2017; and supported members in obtaining $2.2M in new grants (7 projects).
The Healthy Pregnancy strategic priority is common to a number of the initiatives that IHDCYH has led, co-led or supported between 2013 and 2019. These include: HeLTI, the Preterm Birth Initiative, CEEHRC, the Applied Chairs in Reproductive and Child Health Services and Policy ResearchFootnote 5, and CIHR's Integrated Cannabis Research Strategy. IHDCYH's key effort to address this strategic priority was to fund Clinician-Investigator Teams in Obstetrics and Maternal-Fetal Medicine, which are supporting early- and mid-career investigators to overcome research capacity challenges in this area of research and tackle some of the key issues to improve the health of mothers and infants across Canada. Some of the outcomes of this investment are discussed in the Contributions to Capacity Building section of this report.
For the Healthy Public Policy and Systems Integration research investment theme, IHDCYH's key activities in supporting research into Integrating Child and Youth Health Services include the institute's involvement in four cross-cutting CIHR initiatives—Transitions in Care Initiative (TiC), Community-Based Primary Health Care (CBPHC) Innovation teams, the Pan Canadian Strategy for Patient-Oriented Research Networks in Primary and Integrated Health Care Innovations (SPOR PIHCI), Collaborative Health Research Projects: Special Call - Artificial Intelligence, Health and Society—as well as the Applied Chairs in Reproductive and Child Health Services and Policy Research. Investment to date within the SPOR PIHCI initiative that is relevant to IHDCYH has totaled $16.65M including matching funds from external partners through a range of funding opportunities released between 2013 and 2017. For example, a SPOR PIHCI Quick Strike-funded project by Dr. Shelley Doucet from University of New Brunswick and Dr. Rima Azar from Mount Allison University and their team resulted in the creation of NaviCare/SoinsNavi, a pediatric patient navigation service for children with complex care needs. Since the service opened two years ago, it has served over 145 families and Dr. Doucet and Dr. Azar have been evaluating the service and identifying barriers and gaps in the services available to families, information that is used to strengthen NaviCare/SoinsNavi. The SPOR PIHCI New Brunswick and PEI Networks have also been working together to identify how they can create a provincial-level Child Health Profile and Birth Cohort from available administrative data that would be for reporting and outcome monitoring of intervention programs.
Between 2013 and 2017, investments to address IHDCYH's Mental Health strategic priority have been made through Partnerships for Health System Improvement (PHSI) Mental Health Priority Announcement, as well as collaboration on three multi-institute strategic initiatives focused on Mild Traumatic Brain Injury, Pathways to Health Equity for Aboriginal Peoples and eHealth Innovations. Within the Mild Traumatic Brain Injury initiative, research by Dr. Carolyn Emery and her team at the University of Calgary's Sport Injury Prevention Research Centre has prompted Hockey Canada to ban body checking for players under 12 years of age, which has resulted in a 64% reduction in concussion risk and 50% reduction in injury risk overall.
Other examples of the outcome of IHDCYH's knowledge creation and translation investments and activities in the policy, practice and public domains include: guidelines for safe and active transport to schools; baseline scorecard of the mental health and addictions system; new methods for doing cost analysis to estimate the burden of preterm birth and economic impact of improving outcomes; regional primary health care portraits across British Columbia, Ontario and Nova Scotia; solutions to prevent firearm injuries; programs and interventions designed to address the role of poor nutrition, stress, and other maternal adversity in the health of women and their developing babies; tele-mental health services for First Nations communities; and child and youth injury reduction.
Key informants expressed mixed views regarding the effectiveness of IHDCYH's national and international partnerships. There was consensus that convener and catalyst activities were just as important as the funding role given the limited resources at the discretion of the institute. Suggested partnerships and collaborations with Children's Healthcare Canada (formerly CAPHC), Maternal Infant Child and Youth Research Network (MICYRN), and the Canadian Institute for Advanced Research (CIFAR) – especially its Child and Brain Development Program should be actively considered. In terms of international partnerships, key informants suggested partnerships with international Non-Government Organizations, Welcome Trust, Bill and Melinda Gates Foundation, NIH, European clinical trial groups, charities, philanthropies, civil society groups, professional groups, and the Pediatric Trials Network in the US. Further, there was agreement that international partners have the opportunity to co-fund HeLTI if approached strategically.
In terms of knowledge advancement and translation activities, key informants suggest finding clever ways to include knowledge translation in grants. Examples include funding solution-oriented research, such as drawing on lessons learned from Environmental Influences on Child Health Outcomes (ECHO) study at NIH, and looking to include intervention components into research through natural experiments, prevention trials, and pilot studies that bridge the gap between fundamental and applied research. Concerted efforts to improve transdisciplinary team-based research was a consistent recommendation, including clinical scientists, social scientists, trial researchers, policy makers, and early career investigators (ECIs) into the design of these grants for increased chances of knowledge translation.
2. Contributions to Building Capacity
IHDCYH has implemented a comprehensive strategy to increase capacity across within its mandate by embedding training and capacity building in all its activities, providing support across research themes and the research career pipeline, addressing key areas of need in under-represented fields, and addressing barriers to entry into researchFootnote 6. The following are key examples of IHDCYH's investments and outcomes in capacity-building by career-stage.
For trainees, training/capacity building is embedded as a requirement into all major IHDCYH funding opportunities, which ensures trainees are exposed to and involved in research areas across IHDCYH's mandate. IHDCYH also supports the CIHR Travel Award program and provides funds for research trainees (master's and doctoral students, and postdoctoral fellows) to present their own research at meetings and conferences related to the Institute's mandate.
For early career investigators (ECIs), IHDCYH's two key programs are:
- Early Career Investigators in Maternal, Reproductive, Child and Youth Health program, which supports research related to any area of IHDCYH's mandate. The program funded its first cycle of ECIs in 2017, a second cycle in 2018, with a third cycle in 2019 currently underway. Each cycle is a partnership between IHDCYH and other CIHR institutes with an additional funding match provided by partners obtained by the applicants, most often their host institution. In 2017, the competition was a partnership between IHDCYH, ICR, ICRH, IIPH, IMHA, INMHA and INMD with each of the partnering institutes providing grants of $75,000 over three years to support research within maternal-child-youth health relevant to each institute's mandates. The total funding available from CIHR in 2017 was $1.7M, which was matched 1:2 by the applicants' host institutions to fund 26 early career investigators. In the 2018 competition, the funding was changed to $105,000 per grant from CIHR with a 1:1 match from the applicant partners. The CIHR institutes supporting the 2018 round were IHDCYH, ICRH, IHSPR, III, IIPH, IMHA and INMHA for a total of $1.7M from CIHR and 17 early career investigators funded.
- SickKids-IHDCYH New Investigators in Child and Youth Health: Launched in 2001, the program is partnership between IHDCYH and SickKids that provides 6 grants each year of $300,000 each over 3 years. During this time 160 grants totaling $30M have been awarded, of which 37 grants totaling $9.1M were awarded during Dr. Lee's tenure. Recent recipients of a SickKids-IHDCYH New Investigators in Child and Youth Health grant include: Dr. Simone N. Vigod (2014), whose research focuses on women with mental health issues and their journeys prior to, during, and after pregnancy, and who now leads the Reproductive Life Stages Program at the Women's College Hospital, Toronto; and Dr. Pia Wintermark (2013), who investigates brain damage in newborns and is Director of the NeoBrainLab at Montreal Children's Hospital.
In addition, IHDCYH provides educational activities and resources to trainees and ECIs through the following activities: ECI workshops, Summer Institutes, planning and dissemination grants, and conference-related activities such as poster sessions and information webinars.
For mid-career researchers, IHDCYH has funded two programs to address key capacity gaps within its mandate area: CIHR Applied Chairs in Reproductive, Child and Youth Health, and the Clinician-Investigator Teams in Obstetrics and Maternal-Fetal Medicine.
At the end of 2012, IHDCYH funded six Applied Health Chairs in Reproductive and Child Health Services and Policy Research to address barriers to the generation of applied health services and policy research and its translation to decision-makers in the domain of reproductive, child and youth health. The program seeks to bridge this gap by supporting mid-career faculty (between 5-15 years of experience) who: conduct reproductive, child and youth health services and policy research; are dedicated to working with decision makers to frame their research questions and interpret their results; and train and mentor students, fellows, junior faculty and others seeking career opportunities in the field of applied health services and policy research. The six Chairs were funded with a total investment of $5.53M over five years: each Chair received a $100K salary contribution and $85K allowance for research, education mentoring and knowledge translation each year.
To date, reporting data indicate that the Applied Chairs have increased research capacity as well as produced high-impact research that has changed health services and policy in Canada. At their mid-point, the Applied Chairs had produced 172 peer reviewed manuscripts (95 of which included at least one trainee as author); given 208 presentations, lectures and invited talks; and supervised or mentored 117 undergraduate, graduate and postgraduate trainees, with over 20 of those trainees now working as independent researchers.
In addition to increase research capacity and output, the translation and application of the research findings are having an impact on the policy, practice and public domain across the life-course from pregnancy to youth. Table 1 provides some examples of impact.
Table 1. Highlights of Applied Chair Impacts on Policy, Practice and Public
| Policy Domain | Dr. KS Joseph from UBC completed several projects in collaboration with Perinatal Services BC. Several of his findings had significant implications for clinicians, ethicists and health policy makers including:
|
| Practice Domain | Dr. Prakesh Shah's work at Mount Sinai Hospital through the International Network for Evaluation of Outcomes (iNeo) in neonates identified best practices to improve outcomes for low birth weight infants. iNeo has been able to develop and maintain meaningful collaborations and partnerships with investigators from the Canadian Neonatal Network, new partnerships with Network Directors and Leaders from nine countries, and is currently undergoing extensions to include national networks from four other countries. |
| Public Domain | Dr. Roberta Woodgate and her team worked with a local filmmaker to create a 3-part video series that raises awareness of the experiences of First Nations families of children with disabilities. They also organized a Summit which included diverse stakeholders who participated in the project to present findings and encourage shifts in policies. Their innovative KT approach has resulted in requests from numerous agencies, including Health Canada, for guidance on KT best practices. Working with the Canadian Association of Paediatric Health Centres (CAPHC, now Children's Healthcare Canada), Dr. Woodgate also presented a webinar in 2014 exploring experiences of families of children with complex needs, which had over 200 virtual local, national and international attendees and was one of three top webinars hosted by the CAPHC in 2014. |
The Clinical-Investigator Teams in Obstetrics and Maternal-Fetal Medicine (C-I Teams) are a new approach to both build capacity, as well as advance knowledge creation and translation. The program is designed to encourage clinicians to undertake research and remedy the lack of early- and mid-career clinician investigators in the field of obstetrics and maternal-fetal medicine. By providing practicing clinicians who have limited protected time to undertake research with the resources they need to establish teams, the program increases their capacity to conduct research. A total of five teams were funded in 2016 for five years and all are focusing on improving maternal and infant perinatal outcomes. The total funding provided by IHDCYH for this program was $3.73M over five years, which was matched 1:1 by each team's institution(s).
To date, the five teams have been highly productive in terms of both building research capacity as well as advancing knowledge. By the end of the second year of their grants, the five teams have had their C-I Team principal investigators maintain 60% clinical time; hired research staff (average of 2.0 full-time equivalent per team); engaged trainees (average of four per team); and secured host institution support (matching funds, research space and access to research and administrative support services). In terms of knowledge creation, the five teams combined had published 85 journal articles, given 34 invited presentations and 96 peer-adjudicated presentations, such as poster and/or oral presentations at conferences. The teams have also been highly successful in gaining additional funding and collaborating with others in the obstetrics and maternal-fetal medicine field. C-I Team principal investigators are Principal Applicants on 14 successful grant applications with average funds of $70,943 from sources including CIHR, FRQS and Quebec Health Ministry. Furthermore, they are Co-Applicants on 12 successful grant applications with average funds of $4.4M from sources including CIHR and Health Canada.
IHDCYH investments in capacity building from the ISI budget remained relatively stable between approximately $2.4M and $3.1M from 2012-13 to 2017-18 with the exception of 2015-16 and 2016-17 due to the reallocation of funds to RAF initiatives (Figure 11, Appendix 3). These investment levels underestimate the extent of IHDCYH investments in capacity building as almost all of the Institute's funding mechanisms include a training component and/or grant evaluation criteria included a specific focus on ECIs and trainees. The proportion of CIHR-funded researchers under IHDCYH's mandate steadily increased from 9% in 2000-01 to 21% in 2017-18 (Figure 12, Appendix 3).
IHDCYH, under Dr. Shoo Lee, also leveraged other CIHR capacity building programs by investing $4.4M in the CIHR Strategic Training Initiative in Health Research (STIHR) Program between 2012-13 and 2014-15. This funding was used to support several grants for health research training programs including the Canadian Child Health Clinician Scientist Program (CCHCSP) and the CIHR Training Program in Reproduction, Early Development, and their Impact on Health (REDIH). CCHCSP is an ongoing program that trains and supports new clinician-investigators in child and youth health research at the PhD, postdoctoral, and early-career investigator career stages, providing support and multidisciplinary networking for practicing clinicians from diverse backgrounds, including medicine, nursing, psychology, physical and occupational therapy, and dietetics. The goal of the REDIH program was to increase the number of graduate students, postdoctoral fellows, and clinician-scientists in Canada receiving comprehensive training in reproductive and early developmental biology and health.
Key informants expressed mixed views regarding the effectiveness of IHDCYH's capacity building approach, with some expressing appreciation and some expressing disappointment. Those key informants expressing disappointment would like future capacity building investments to include financial, mentorship and training components. Mechanisms for improvement include enhancing professional development to prepare researchers for leadership roles in diverse sectors (e.g. national mentorship programs outside of academic centers), increasing mentorship to effectively navigate the funding landscape, and enhancing professional networking (e.g. connecting researchers with non-government organizations and industry). Here, it is important to note that CIHR's Strategic Action Plan on Training has identified similar challenges to career training and support and has developed a plan to address these challenges. Key stakeholders, however, would like to see a greater openness for IHDCYH to collaborate with other existing capacity-building programs (CCHCSP), continue to invest in Network Environments for Indigenous Health Research (NEIHR), and look to leverage future opportunities under the Strategic Action Plan on Training. One key informant particularly well informed of IHDCYH capacity building initiatives felt as though IHDCYH underperformed in the area of capacity building when compared to other CIHR Institutes. Further, another key informant suggested supporting ECIs in large studies and also supporting them at the end of this stage to support their transition to mid-career investigators following NIH's model. The need for improved metrics to measure impacts of funding opportunities (e.g. integrating performance of ECIs on team grants) was mentioned as being important for CIHR as a whole moving forward.
C. Convener and Catalyst
During Dr. Lee’s tenure, IHDCYH served as a champion and convener for research and knowledge translation among the Institute’s national and international stakeholder communities. IHDCYH maintained and forged strong partnerships and networks with other CIHR Institutes (see Figure 6 in Appendix 3), governments, not-for-profit organizations, research communities, and end-user groups. For example, IHDCYH successfully brought together the World Health Organization, the National Natural Science Foundation of China, the Department of Biotechnology of India, and the South African Medical Research Council to launch the HeLTI Linked International Intervention Cohorts. IHDCYH advanced research in its area by investing in initiatives that include the Canadian Urban Environmental Health Research Consortium (CANUE), which brought together large research groups and networks in the area of Environmental Health (e.g., CHILD, MIREC, ReACH, BORN, and TARGetKids!).
IHDCYH strengthened their convener catalyst role by focusing on their partnerships. IHDCYH partnered with provincial health research funding agencies and key provincial healthcare delivery organizations to improve community-based primary and integrated health care (e.g. SPOR Network in Primary and Integrated Health Care Innovations). Capacity building was supported in areas such as the Applied Chairs in Reproductive, Child and Youth Health Clinician-Investigator Teams in Obstetrics and Maternal-Fetal Medicine, and Early Career Investigators in Maternal, Reproductive, Child and Youth Health programs by partnerships with a range of organizations. Additionally, IHDCYH forged in-kind partnerships to connect its stakeholder communities, build capacity, and promote knowledge translation (e.g. ongoing relationship with Children’s Healthcare Canada).
IHDCYH regularly consulted its stakeholder communities, shared information with, engaged, and connected its stakeholder communities via national conferences, social media (e.g., the IHDCYH Talks Video Competition, Facebook, Twitter, IHDCYH’s webpages), and public facing events (e.g., Café Scientifique sessions, Facebook Live Events and ministerial announcements).
A key communication strategy of IHDCYH has been to develop an active and diverse web/online and social media presence to ensure that stakeholders are both informed and connected, as well as to support knowledge translation activities across the institute’s community. Through these efforts the institute keeps stakeholders (researchers, trainees, parents/patients, health professionals, advocacy groups, research institutions, and decision makers) informed of initiatives, funding opportunities and news, featured research and other resources available on their website, training courses, workshops, job opportunities and conferences. These means include their website (41K views/year), Twitter account (2,010 followers; 51K views/month), and eBulletin (719 subscribers, 41.2% open rate). In particular, IHDCYH has focused on highlighting and celebrating researcher impact stories through their website, ebulletin and Twitter. The Institute further informs and connects with stakeholders by leveraging CIHR’s social media (Twitter, Facebook and LinkedIn) and ebulletin (ACCESS and other Institutes' newsletters) and with partner social media and communication channels.
Launched in 2014, the annual IHDCYH Talks Video Competition is an innovative communication and knowledge translation mechanism using YouTube to improve knowledge translation and demonstrate the impact evidence can and does have on maternal, reproductive, child and youth health in Canada. Independent researchers, trainees (all research pillars and career levels), representatives from Canadian non-governmental, and/or not-for-profit organizations and knowledge users, including members of the public, are eligible to submit a video, with up to $15,000 in total for winner and runner up prizes each year. Submitted videos must demonstrate a clear, evidence-based message related to IHDCYH’s mandate and/or strategic priorities. The range of topics covered include: healthy pregnancy, adverse childhood experiences (ACE) and child sexual abuse prevention, youth and maternal mental health, Indigenous experiences, cultural experiences, disabilities, pain management, common childhood health concerns (vomiting, diarrhea, cough, ear pain), ASD, chronic disease prevention and treatment (childhood obesity, diabetes, arthritis), physical activity, nutrition, anaphylaxis, FASD, sleep, and importance of the early years. In 2018, 27 applications were received and 6 prizes awarded (CIHR-Institute of Infection and Immunity (III) provided funds to allow an additional prize to be awarded). Successful videos are posted on IHDCYH’s YouTube channel, CIHR and IHDCYH’s webpage, and promoted through social media (Twitter, Facebook and LinkedIn) and IHDCYH’s bi-weekly e-bulletin. To date, the videos have been viewed over 240K times.
IHDCYH has successfully leveraged many stakeholder relationships under Dr. Lee’s leadership. Notably, annual external partner contributions in funding opportunities related to IHDCYH’s mandate increased from $8M in 2012-13 to $12.6M in 2017-18, with a peak of $14.1M in 2016-17 (Figure 15, Appendix 3). IHDCYH also leveraged their more intangible relationships, such as those developed with professional societies to help them disseminate knowledge products as well as build capacity.
IHDCYH’s average leverage ratio for the period of 2012-13 to 2017-18 is 0.51 (Figure 16, Appendix 3). This means that between 2012-13 and 2017-18, for every $100 IHDCYH invested, partners invested an average of $51. The leverage ratio was fairly stable at an average of 0.39 between 2012-13 and 2014-15. There was a steep increase to 0.72 in 2015-16. The leverage ratio decreased in 2016-17 to 0.46 and then increased to 0.71 in 2017-18. It is worth noting that the leverage ratio increase in 2015-16 may be due to a significant reduction in the IHDCYH ISI budget from $7.8M in 2014-15 to $2.5M in 2015-16, while the level of prior IHDCYH ISI and partner funding is maintained.
Key informants as well as the Panel held a mixed consensus regarding IHDCYH’s ability to build and leverage partnerships. They identified an opportunity for the next SD to leverage partnerships and collaborations at both the national and international level as well as within various sectors (e.g., NGOs) and existing networks (e.g., MICYRN). Successfully connecting to build and leverage partnerships within Indigenous communities was described as a challenge. It was suggested that IHDYCH leverage existing partnership programs such as CCHCSP in the future. Additionally, there is an agreed upon importance that IHDCYH continue to foster networking and connection between stakeholders through various avenues such as hosting meetings and video competitions.
D. Operational Effectiveness
Under Dr. Lee’s leadership, and through an unprecedented period of financial instability and change at CIHR, IHDCYH successfully used its strategic budget to develop initiatives and funding opportunities to address all of its strategic themes and enabling tactics. In addition, IHDCYH’s host institution, the Lunenfeld-Tanenbaum Research Institute, received $1M annually through CIHR’s Institute Support Grant (ISG) to establish and sustain Institute activities and events; if the annual ISG allotment is not completely expended in a given fiscal year, the balance can be transferred to the next fiscal year. During this period, IHDCYH spent an average of 20% of its ISG budget each year on Institute Strategic Development costs (e.g. costs related to consultations for the development of strategic initiatives, participating in conferences and workshops, and hosting Institute Advisory Board meetings). Since 2011-12, IHDCYH spent an annual average of $845K of its ISG on Institute operations (e.g. salaries and benefits, travel of SD and staff in Canada and internationally to support strategic activities, rental of office space) (Figure 17 in Appendix 3). As of 2017-18, IHDCYH has accumulated a surplus of approximately $577K in order to both ensure sufficient funding for the final four months of its mandate, a period for which the estimated expenditures will exceed the ISG allotment for that short period, and to financially support the transition period that will follow the end of Dr. Lee’s tenure – as a leading practice (Figure 18 in Appendix 3).
Dr. Lee was able to accomplish IHDCYH’s goals in an efficient manner despite difficult operational and financial circumstances from the outset. During Dr. Lee’s first term as SD, CIHR changed the nature and the extent of the support it provides to the institutes. Prior to July 2015, the institutes were supported by full-time Ottawa-based Institute Staff (OBIS) in addition to the host institute staff. In the case of IHDCYH, two full-time equivalent (FTE) CIHR employees were an integral part of the team and provided optimal communications, negotiations and interactions with other CIHR branches in Ottawa, as well as providing 'generalist' support to the institute across its range of activities. These individuals also provided a link between the Institute and the Ottawa-based branches to help ensure stability and corporate memory across Institute SD transitions. As part of the Institute Modernization introduced in 2014 by CIHR’s Governing Council, it was decided that the Ottawa-based Institute Staff would be integrated into other CIHR portfolios, and Integrated Institute Teams (IIT) were created to support Institutes. This matrix management model (integrated teams comprised of functional staff from various Branches across CIHR Portfolios) provides advice and some support to each Institute as a part of the integrated team. Each IIT team member works with multiple Institutes, as well as continuing with the responsibilities of their role at CIHR. The workload of the Institute increased in an important fashion with the implementation of these changes and all this was to be done with the same annual ISG budget. In order to mitigate (in part) this additional workload, the Institute increased its host institution staff from 2.5 FTE (under the OBIS model to 2014) to 4.0 FTE (under the IIT model from 2015), with the creation an additional full-time position in 2015, as well as increasing the Executive Assistant and Finance Manager support.
V. Appendices
Appendix 1: IHDCYH Review Panel Members' Affiliation and Conflict of Interest Declaration
Chair: Frank Gavin, CHILD-BRIGHT Citizen Engagement Director; Founder and Director, Canadian Family Advisory Network (CFAN)
Panel Members:
- Meghan Azad, Assistant Professor, Pediatrics & Child Health and Community Health Sciences, University of Manitoba; Research Scientist, Children's Hospital Research Institute of Manitoba
- Sandra Davidge, Director, Women's and Children's Health Research Institute (WCHRI); Professor, University of Alberta
- Mark Hanson, Professor, Faculty of Medicine, University of Southampton, UK; Founder, member, and ex-president of International Society for DOHaD
- Patrick McGrath, VP Research, Innovation and Knowledge Translation IWK and Nova Scotia Health Authority; Professor, Psychology, Pediatrics and Psychiatry, Dalhousie University
- Anne Monique Nuyt, Head, Division of Neonatology, CHU Sainte-Justine; Head, Center of Excellence in Neonatology, CHU Sainte-Justine; Professor of Pediatrics, Université de Montréal
| Panel Member | Conflict of Interest Declaration |
|---|---|
| Frank Gavin | Confirmed no real, apparent or potential conflict(s) of interest with respect to his involvement with the Review Panel |
| Meghan Azad | Co-Applicant & Co-Lead, Operating Grant: Environmental Urban Health Research Consortium (2016-2021), Canadian Urban Environmental Health (CANUE) Research Consortium, $4.165M |
| Sandra Davidge | Confirmed no real, apparent or potential conflict(s) of interest with respect to his involvement with the Review Panel |
| Mark Hanson | Confirmed no real, apparent or potential conflict(s) of interest with respect to his involvement with the Review Panel |
| Patrick McGrath | Confirmed no real, apparent or potential conflict(s) of interest with respect to his involvement with the Review Panel |
| Anne Monique Nuyt | Confirmed no real, apparent or potential conflict(s) of interest with respect to his involvement with the Review Panel |
Appendix 2: Overview of Data Sources and Methods
| Data source | Description |
|---|---|
| Situational Analysis (SA) |
|
| Key informant interviews |
|
| Bibliometric Analysis |
|
Appendix 3: Key Figures
Figure 1: Percent of World Publications
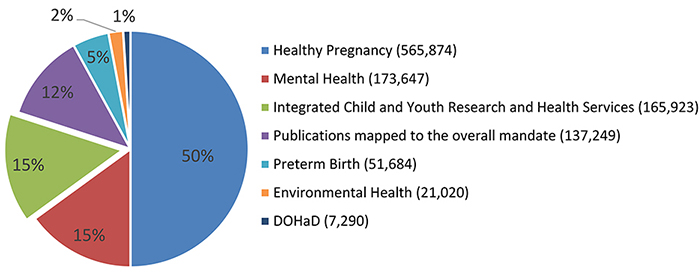
Figure 1 – Long Description
| Percent of Publications | |
|---|---|
| Healthy Pregnancy (565,874) | 50% |
| Mental Health (173,647) | 15% |
| Integrated Child and Youth Research and Health Services (165,923) | 15% |
| Publications mapped to the overall mandate (137,249) | 12% |
| Preterm Birth (51,684) | 5% |
| Environmental Health (21,020) | 2% |
| DOHaD (7,290) | 1% |
Figure 2: Average of Relative Citations in IHDCYH’s mandate
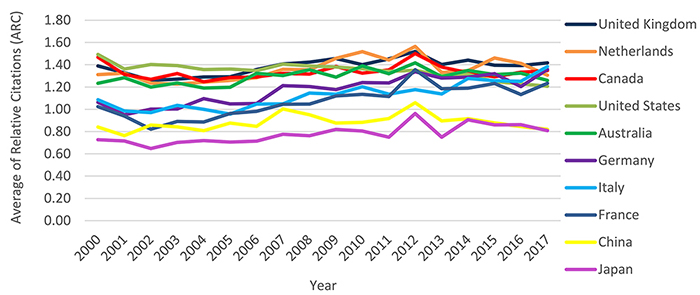
Figure 2 – Long Description
| 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2011-2017 | Ranking | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| United Kingdom | 1.39 | 1.33 | 1.26 | 1.27 | 1.29 | 1.29 | 1.36 | 1.41 | 1.42 | 1.46 | 1.40 | 1.45 | 1.52 | 1.40 | 1.44 | 1.40 | 1.39 | 1.42 | 1.40 | 1 |
| Netherlands | 1.31 | 1.32 | 1.24 | 1.23 | 1.24 | 1.26 | 1.28 | 1.36 | 1.36 | 1.46 | 1.52 | 1.44 | 1.56 | 1.33 | 1.35 | 1.46 | 1.41 | 1.31 | 1.38 | 2 |
| Canada | 1.47 | 1.31 | 1.27 | 1.32 | 1.25 | 1.29 | 1.29 | 1.32 | 1.32 | 1.38 | 1.32 | 1.35 | 1.50 | 1.38 | 1.33 | 1.29 | 1.33 | 1.35 | 1.34 | 3 |
| United States | 1.49 | 1.36 | 1.40 | 1.39 | 1.36 | 1.36 | 1.35 | 1.41 | 1.39 | 1.38 | 1.36 | 1.34 | 1.35 | 1.31 | 1.32 | 1.25 | 1.23 | 1.21 | 1.33 | 4 |
| Australia | 1.23 | 1.28 | 1.20 | 1.24 | 1.19 | 1.20 | 1.32 | 1.30 | 1.36 | 1.29 | 1.39 | 1.32 | 1.42 | 1.29 | 1.35 | 1.31 | 1.32 | 1.26 | 1.31 | 5 |
| Germany | 1.06 | 0.95 | 1.00 | 1.00 | 1.10 | 1.05 | 1.05 | 1.21 | 1.20 | 1.18 | 1.24 | 1.24 | 1.34 | 1.28 | 1.29 | 1.32 | 1.20 | 1.36 | 1.20 | 6 |
| Italy | 1.09 | 0.99 | 0.97 | 1.04 | 1.00 | 0.96 | 1.05 | 1.05 | 1.15 | 1.14 | 1.20 | 1.14 | 1.18 | 1.14 | 1.28 | 1.26 | 1.25 | 1.38 | 1.15 | 7 |
| France | 1.02 | 0.94 | 0.82 | 0.89 | 0.89 | 0.96 | 0.98 | 1.05 | 1.05 | 1.12 | 1.13 | 1.12 | 1.36 | 1.18 | 1.19 | 1.23 | 1.13 | 1.23 | 1.10 | 8 |
| China | 0.84 | 0.76 | 0.86 | 0.84 | 0.81 | 0.88 | 0.85 | 1.00 | 0.95 | 0.88 | 0.88 | 0.92 | 1.06 | 0.90 | 0.92 | 0.88 | 0.85 | 0.82 | 0.89 | 9 |
| Japan | 0.73 | 0.72 | 0.65 | 0.70 | 0.72 | 0.71 | 0.71 | 0.78 | 0.76 | 0.82 | 0.80 | 0.75 | 0.96 | 0.75 | 0.91 | 0.86 | 0.86 | 0.81 | 0.78 | 10 |
| World | 1.15 | 1.08 | 1.07 | 1.07 | 1.07 | 1.07 | 1.08 | 1.10 | 1.09 | 1.09 | 1.07 | 1.07 | 1.07 | 1.04 | 1.04 | 1.00 | 0.99 | 0.98 | 1.05 |
Figure 3: Average of Relative Citations of Canadian Publications by IHDCYH Strategic Priority Area
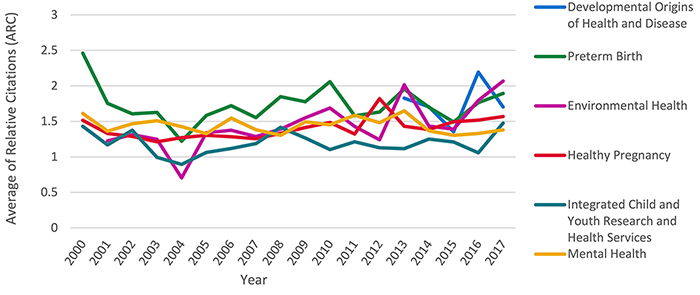
Figure 3 – Long Description
| 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2011-2017 | Ranking | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Developmental Origins of Health and Disease | 1.83 | 1.71 | 1.35 | 2.19 | 1.70 | 1.67 | 4 | |||||||||||||
| Preterm Birth | 2.46 | 1.75 | 1.61 | 1.63 | 1.22 | 1.58 | 1.72 | 1.55 | 1.85 | 1.78 | 2.06 | 1.58 | 1.63 | 1.95 | 1.70 | 1.49 | 1.76 | 1.89 | 1.73 | 2 |
| Environmental Health | 1.23 | 1.31 | 1.25 | 0.70 | 1.34 | 1.38 | 1.29 | 1.39 | 1.55 | 1.69 | 1.43 | 1.24 | 2.02 | 1.43 | 1.39 | 1.80 | 2.07 | 1.53 | 5 | |
| Healthy Pregnancy | 1.51 | 1.33 | 1.29 | 1.21 | 1.27 | 1.31 | 1.28 | 1.26 | 1.33 | 1.41 | 1.48 | 1.32 | 1.82 | 1.43 | 1.38 | 1.49 | 1.52 | 1.57 | 1.43 | 3 |
| Integrated Child and Youth Research and Health Services | 1.43 | 1.17 | 1.38 | 0.99 | 0.89 | 1.06 | 1.12 | 1.19 | 1.41 | 1.27 | 1.10 | 1.21 | 1.13 | 1.12 | 1.25 | 1.21 | 1.06 | 1.48 | 1.20 | 3 |
| Mental Health | 1.61 | 1.36 | 1.47 | 1.51 | 1.43 | 1.33 | 1.55 | 1.38 | 1.30 | 1.49 | 1.45 | 1.59 | 1.48 | 1.65 | 1.37 | 1.30 | 1.33 | 1.38 | 1.43 | 3 |
Figure 4: Average Relative Impact Factor in IHDCYH’s mandate
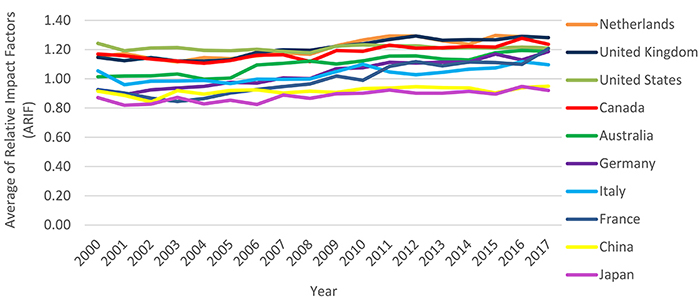
Figure 4 – Long Description
| 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2011-2017 | Ranking | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Netherlands | 1.15 | 1.17 | 1.14 | 1.11 | 1.15 | 1.14 | 1.16 | 1.18 | 1.17 | 1.23 | 1.27 | 1.29 | 1.29 | 1.26 | 1.24 | 1.30 | 1.29 | 1.28 | 1.23 | 1 |
| United Kingdom | 1.15 | 1.12 | 1.15 | 1.12 | 1.12 | 1.13 | 1.18 | 1.20 | 1.19 | 1.22 | 1.24 | 1.27 | 1.29 | 1.26 | 1.27 | 1.27 | 1.29 | 1.28 | 1.23 | 2 |
| United States | 1.24 | 1.19 | 1.21 | 1.21 | 1.19 | 1.19 | 1.20 | 1.19 | 1.18 | 1.22 | 1.23 | 1.23 | 1.23 | 1.21 | 1.21 | 1.21 | 1.22 | 1.21 | 1.21 | 3 |
| Canada | 1.17 | 1.16 | 1.14 | 1.12 | 1.11 | 1.13 | 1.16 | 1.16 | 1.12 | 1.19 | 1.19 | 1.23 | 1.21 | 1.21 | 1.22 | 1.22 | 1.28 | 1.24 | 1.20 | 4 |
| Australia | 1.01 | 1.02 | 1.02 | 1.03 | 1.00 | 1.00 | 1.10 | 1.11 | 1.12 | 1.10 | 1.12 | 1.15 | 1.16 | 1.14 | 1.13 | 1.18 | 1.19 | 1.19 | 1.13 | 5 |
| Germany | 0.92 | 0.89 | 0.92 | 0.94 | 0.95 | 0.98 | 0.97 | 1.01 | 1.00 | 1.07 | 1.08 | 1.11 | 1.11 | 1.11 | 1.11 | 1.17 | 1.13 | 1.19 | 1.06 | 6 |
| Italy | 1.05 | 0.96 | 0.98 | 0.99 | 0.99 | 0.97 | 1.00 | 1.00 | 1.00 | 1.05 | 1.10 | 1.05 | 1.03 | 1.04 | 1.07 | 1.07 | 1.12 | 1.10 | 1.04 | 7 |
| France | 0.93 | 0.90 | 0.87 | 0.85 | 0.87 | 0.90 | 0.93 | 0.95 | 0.96 | 1.02 | 0.99 | 1.08 | 1.12 | 1.09 | 1.11 | 1.11 | 1.10 | 1.21 | 1.02 | 8 |
| China | 0.91 | 0.89 | 0.84 | 0.92 | 0.89 | 0.92 | 0.92 | 0.90 | 0.92 | 0.91 | 0.93 | 0.94 | 0.95 | 0.94 | 0.94 | 0.90 | 0.94 | 0.95 | 0.93 | 9 |
| Japan | 0.87 | 0.82 | 0.83 | 0.87 | 0.83 | 0.85 | 0.82 | 0.89 | 0.87 | 0.90 | 0.90 | 0.92 | 0.90 | 0.90 | 0.91 | 0.90 | 0.95 | 0.92 | 0.88 | 10 |
| World | 1.04 | 1.00 | 1.00 | 1.00 | 1.00 | 1.01 | 1.02 | 1.02 | 1.02 | 1.04 | 1.04 | 1.05 | 1.05 | 1.04 | 1.04 | 1.03 | 1.04 | 1.04 | 1.03 |
Figure 5: Average Relative Impact Factor of Canadian Publications by IHDCYH Strategic Priority Area
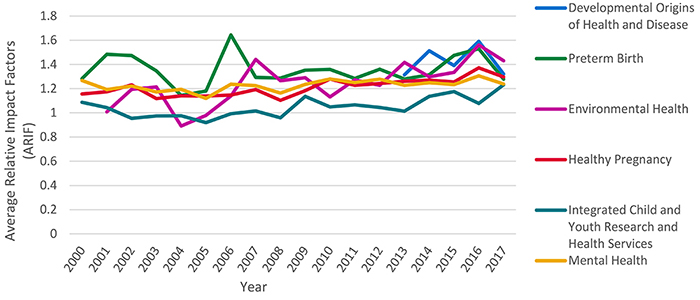
Figure 5 – Long Description
| 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2011-2017 | Ranking | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Developmental Origins of Health and Disease | 1.31 | 1.51 | 1.39 | 1.59 | 1.32 | 1.37 | 4 | |||||||||||||
| Preterm Birth | 1.28 | 1.48 | 1.47 | 1.35 | 1.14 | 1.18 | 1.64 | 1.29 | 1.29 | 1.35 | 1.36 | 1.28 | 1.36 | 1.28 | 1.31 | 1.47 | 1.53 | 1.28 | 1.36 | 2 |
| Environmental Health | 1.01 | 1.19 | 1.21 | 0.89 | 0.98 | 1.14 | 1.44 | 1.27 | 1.29 | 1.13 | 1.27 | 1.23 | 1.42 | 1.30 | 1.34 | 1.56 | 1.43 | 1.30 | 4 | |
| Healthy Pregnancy | 1.16 | 1.17 | 1.23 | 1.12 | 1.14 | 1.14 | 1.15 | 1.19 | 1.10 | 1.18 | 1.28 | 1.23 | 1.24 | 1.26 | 1.27 | 1.25 | 1.37 | 1.30 | 1.23 | 4 |
| Integrated Child and Youth Research and Health Services | 1.09 | 1.04 | 0.95 | 0.97 | 0.98 | 0.92 | 0.99 | 1.02 | 0.96 | 1.14 | 1.05 | 1.07 | 1.04 | 1.01 | 1.14 | 1.18 | 1.08 | 1.23 | 1.08 | 4 |
| Mental Health | 1.27 | 1.19 | 1.22 | 1.17 | 1.19 | 1.12 | 1.24 | 1.22 | 1.16 | 1.23 | 1.28 | 1.25 | 1.28 | 1.23 | 1.25 | 1.23 | 1.31 | 1.24 | 1.24 | 4 |
Figure 6: All IHDCYH Initiatives 2012 to Present
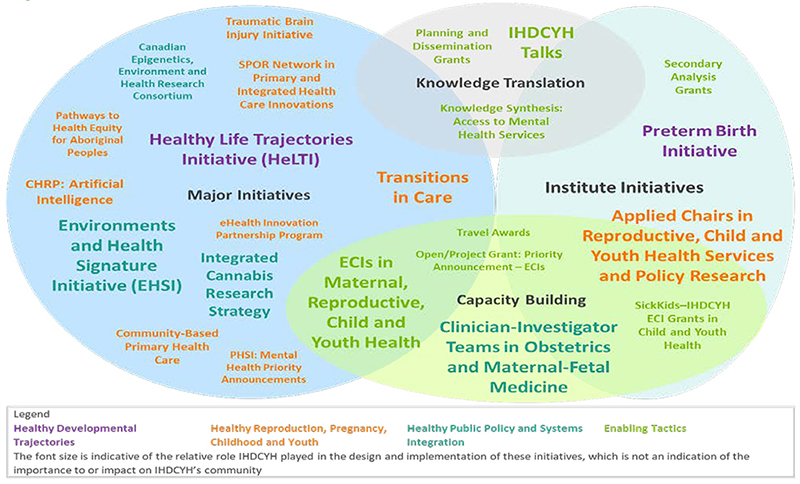
*These initiative also falls under Capacity Building The order of the initiatives in each category of the list is indicative of the relative role IHDCYH played in the design and implementation of these initiatives, which is not an indication of the importance to or impact on IHDCYH's community.
Figure 6 – Long Description
| Major Initiatives | Institute Initiatives | Combination of Major Initiatives and Institute Initiatives | ||
|---|---|---|---|---|
| Knowledge Translation | Capacity Building | |||
| Healthy Developmental Trajectories |
|
|
||
| Healthy Public Policy and Systems Integration |
|
|
||
| Healthy Reproduction Pregnancy Childhood and Youth |
|
|
||
| Enabling Tactics |
|
|
|
|
Figure 7: Annual CIHR Investment in the Mandate of all 13 Institutes
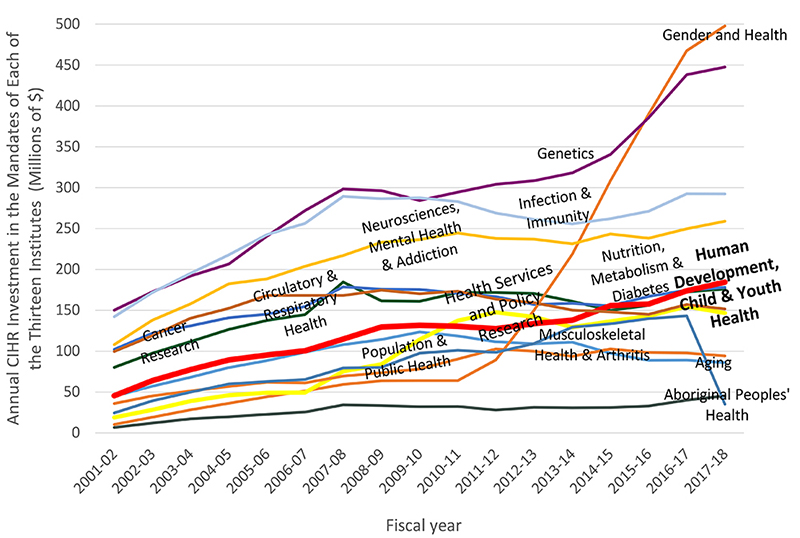
Figure 7 – Long Description
| 2000-01 | 2001-02 | 2002-03 | 2003-04 | 2004-05 | 2005-06 | 2006-07 | 2007-08 | 2008-09 | 2009-10 | 2010-11 | 2011-12 | 2012-13 | 2013-14 | 2014-15 | 2015-16 | 2016-17 | 2017-18 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aboriginal Peoples' Health | $2,139,919 | $6,671,007 | $12,135,931 | $17,174,000 | $19,742,875 | $22,854,683 | $25,351,733 | $34,198,094 | $33,429,217 | $32,132,467 | $32,271,533 | $28,056,449 | $31,249,292 | $30,650,931 | $30,964,204 | $32,839,291 | $40,068,143 | $45,252,668 |
| Aging | $28,024,434 | $44,931,518 | $57,050,531 | $68,051,413 | $79,951,371 | $88,467,602 | $98,831,521 | $108,010,411 | $114,130,755 | $123,437,635 | $118,484,058 | $111,357,253 | $109,097,098 | $110,894,480 | $97,403,006 | $88,540,357 | $89,013,813 | $85,957,061 |
| Cancer Research | $61,686,480 | $80,138,464 | $97,387,259 | $111,858,657 | $126,577,191 | $137,672,077 | $144,724,001 | $184,490,395 | $161,330,701 | $161,038,286 | $171,556,037 | $171,521,059 | $170,515,331 | $161,042,655 | $149,922,615 | $155,976,396 | $172,413,231 | $176,085,836 |
| Circulatory & Respiratory Health | $76,243,639 | $102,118,665 | $121,983,955 | $130,949,429 | $140,852,651 | $145,198,965 | $154,453,965 | $178,642,420 | $175,791,363 | $175,573,279 | $170,843,642 | $166,584,400 | $156,991,790 | $158,564,245 | $155,300,820 | $167,040,873 | $174,610,904 | $177,949,735 |
| Gender and Health | $7,875,116 | $10,300,421 | $19,280,033 | $28,210,404 | $36,064,598 | $44,187,356 | $51,182,999 | $59,245,611 | $63,573,606 | $63,963,815 | $63,974,537 | $89,281,157 | $149,996,334 | $218,692,400 | $308,465,700 | $389,684,077 | $467,496,260 | $497,779,365 |
| Genetics | $118,597,995 | $150,126,260 | $172,382,941 | $191,919,606 | $206,572,337 | $240,609,249 | $271,949,981 | $298,339,945 | $296,403,777 | $284,349,641 | $294,390,755 | $303,928,023 | $308,573,011 | $318,147,719 | $340,516,706 | $385,228,416 | $438,231,699 | $447,515,916 |
| Health Services and Policy Research | $11,360,697 | $18,855,605 | $28,289,289 | $38,820,825 | $46,174,257 | $48,994,239 | $49,368,030 | $75,265,721 | $84,105,448 | $114,330,464 | $137,356,610 | $147,554,312 | $141,992,248 | $129,244,514 | $136,534,015 | $143,154,591 | $154,581,033 | $146,664,008 |
| Human Development, Child & Youth Health | $32,040,855 | $45,428,861 | $63,977,785 | $77,496,050 | $89,249,975 | $95,299,293 | $100,536,611 | $114,851,432 | $129,558,257 | $131,542,595 | $130,543,838 | $127,314,824 | $133,829,463 | $137,921,026 | $155,815,135 | $157,482,297 | $173,885,258 | $184,419,633 |
| Infection & Immunity | $97,532,407 | $142,075,834 | $171,715,800 | $195,231,302 | $217,829,004 | $242,580,100 | $256,326,113 | $289,103,915 | $286,336,960 | $287,441,881 | $282,950,641 | $268,942,600 | $261,113,165 | $255,718,645 | $262,141,782 | $271,196,376 | $292,388,463 | $292,367,666 |
| Musculoskeletal Health & Arthritis | $25,285,282 | $35,905,931 | $45,307,555 | $51,207,110 | $56,773,301 | $62,106,004 | $61,155,105 | $69,436,715 | $73,604,518 | $78,137,921 | $90,433,415 | $102,635,248 | $99,855,250 | $93,666,293 | $102,746,421 | $98,385,548 | $97,784,455 | $94,250,144 |
| Neurosciences, Mental Health & Addiction | $80,058,123 | $107,976,620 | $137,841,709 | $157,846,210 | $182,268,035 | $188,444,569 | $203,900,571 | $216,999,253 | $233,276,868 | $236,358,318 | $244,521,388 | $237,827,851 | $237,024,206 | $231,163,237 | $243,197,089 | $238,064,014 | $249,543,745 | $258,905,385 |
| Nutrition, Metabolism & Diabetes | $78,262,660 | $99,622,776 | $118,871,982 | $140,356,599 | $152,402,916 | $168,122,108 | $168,039,249 | $167,962,832 | $174,587,339 | $170,318,714 | $173,295,436 | $163,583,178 | $159,179,406 | $150,165,929 | $147,879,554 | $144,979,463 | $156,925,156 | $151,528,397 |
| Population & Public Health | $8,302,314 | $24,383,139 | $39,133,321 | $49,809,040 | $59,791,305 | $62,817,496 | $65,165,002 | $79,306,995 | $80,260,646 | $97,465,473 | $100,969,342 | $98,459,475 | $109,321,278 | $129,291,047 | $133,401,598 | $139,625,195 | $143,094,290 | $34,972,867 |
| Total | $369,833,297.00 | $494,540,211.00 | $586,826,186.00 | $646,850,893.00 | $704,689,215.00 | $758,146,346.00 | $799,646,533.00 | $926,716,411.00 | $916,875,687.00 | $929,144,803.00 | $966,828,661.00 | $950,729,984.00 | $940,773,074.00 | $943,955,267.00 | $959,845,009.00 | $972,822,921.00 | $1,024,248,878.00 | $1,035,405,341.00 |
Figure 8: CIHR Investment in IHDCYH Mandate by CIHR Theme
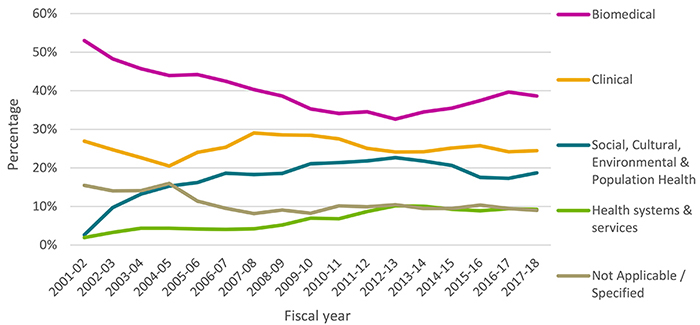
Figure 8 – Long Description
| Primary Theme | 1999-00 | 2000-01 | 2001-02 | 2002-03 | 2003-04 | 2004-05 | 2005-06 | 2006-07 | 2007-08 | 2008-09 | 2009-10 | 2010-11 | 2011-12 | 2012-13 | 2013-14 | 2014-15 | 2015-16 | 2016-17 | 2017-18 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Biomedical | 66% | 66% | 53% | 48% | 46% | 44% | 44% | 42% | 40% | 39% | 35% | 34% | 35% | 33% | 34% | 35% | 37% | 40% | 39% |
| Clinical | 20% | 20% | 27% | 25% | 23% | 20% | 24% | 25% | 29% | 29% | 28% | 28% | 25% | 24% | 24% | 25% | 26% | 24% | 24% |
| Social, Cultural, Environmental & Population Health | 0% | 3% | 10% | 13% | 15% | 16% | 19% | 18% | 19% | 21% | 21% | 22% | 23% | 22% | 21% | 18% | 17% | 19% | |
| Health systems & services | 0% | 2% | 3% | 4% | 4% | 4% | 4% | 4% | 5% | 7% | 7% | 9% | 10% | 10% | 9% | 9% | 9% | 9% | |
| Not Applicable / Specified | 14% | 13% | 15% | 14% | 14% | 16% | 11% | 10% | 8% | 9% | 8% | 10% | 10% | 10% | 9% | 9% | 10% | 9% | 9% |
Figure 9: CIHR Investment in IHDCYH’s Strategic Priorities
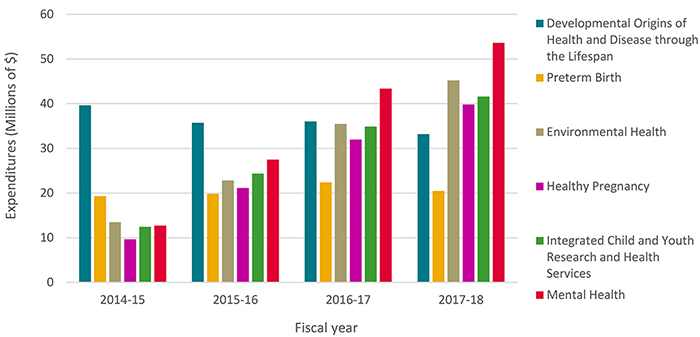
Figure 9 – Long Description
| Strategic Priorities | 2014-15 | 2015-16 | 2016-17 | 2017-18 |
|---|---|---|---|---|
| Developmental Origins of Health and Disease through the Lifespan | $39,662,241.00 | $35,748,667.71 | $36,036,765.89 | $33,191,478.00 |
| Preterm Birth | $19,294,525.00 | $19,833,302.00 | $22,379,869.00 | $20,494,895.00 |
| Environmental Health | $13,497,558.00 | $22,818,520.00 | $35,481,516.69 | $45,218,475.50 |
| Healthy Pregnancy | $9,654,838.00 | $21,121,318.00 | $31,970,063.03 | $39,802,998.67 |
| Integrated Child and Youth Research and Health Services | $12,436,714.00 | $24,344,808.00 | $34,876,351.73 | $41,597,831.47 |
| Mental Health | $12,743,726.00 | $27,508,244.00 | $43,376,268.73 | $53,636,419.50 |
Figure 10: IHDCYH Institute-Specific Initiative (ISI) Budget Spending
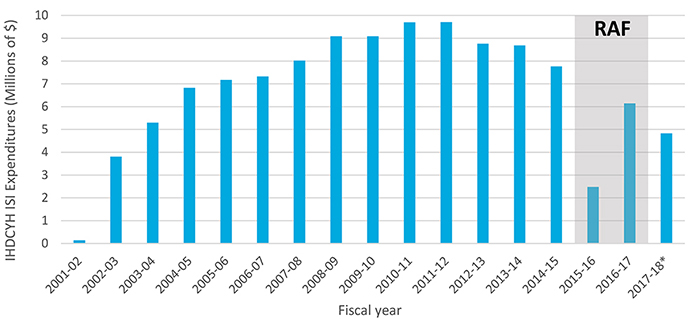
* Starting in 2017-18, Institutes regained full control of their ISI, while being required to maintain previous RAF commitments.
Figure 10 – Long Description
| Fiscal Year | 2001-02 | 2002-03 | 2003-04 | 2004-05 | 2005-06 | 2006-07 | 2007-08 | 2008-09 | 2009-10 | 2010-11 | 2011-12 | 2012-13 | 2013-14 | 2014-15 | 2015-16 | 2016-17 | 2017-18* |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IHDCYH ISI | $143,183.00 | $3,813,540.00 | $5,304,668.00 | $6,821,283.00 | $7,174,746.00 | $7,328,658.00 | $8,020,865.00 | $9,082,501.00 | $9,085,693.00 | $9,702,670.00 | $9,712,219.00 | $8,757,776.00 | $8,690,164.00 | $7,766,692.00 | $2,484,063.00 | $6,146,633.00 | $4,834,540.00 |
| RAF | 10000000 | 10000000 |
Figure 11: Investment in Capacity Building out of IHDCYH’s ISI Budget
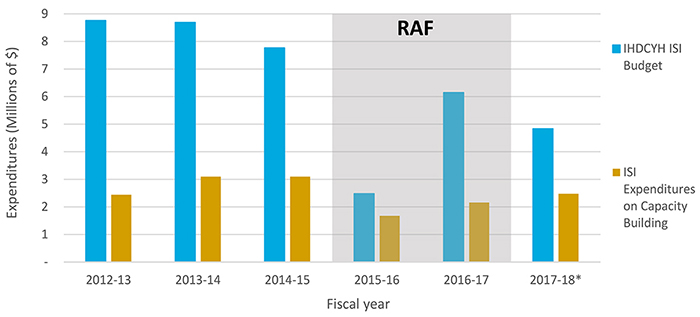
* Starting in 2017-18, Institutes regained full control of their ISI, while being required to maintain previous RAF commitments.
Figure 11 – Long Description
| 2012-13 | 2013-14 | 2014-15 | 2015-16 | 2016-17 | 2017-18* | |
|---|---|---|---|---|---|---|
| IHDCYH ISI Budget | $8,757,776.00 | $8,690,164.00 | $7,766,692.00 | $2,484,063.00 | $6,146,633.00 | $4,834,540.00 |
| ISI Expenditures on Capacity Building | $2,440,667.00 | $3,097,357.71 | $3,097,686.00 | $1,678,174.00 | $2,158,488.00 | $2,473,206.00 |
| RAF | 9000000 | 9000000 |
Figure 12: Percentage of Funded Researchers under IHDCYH’s mandate
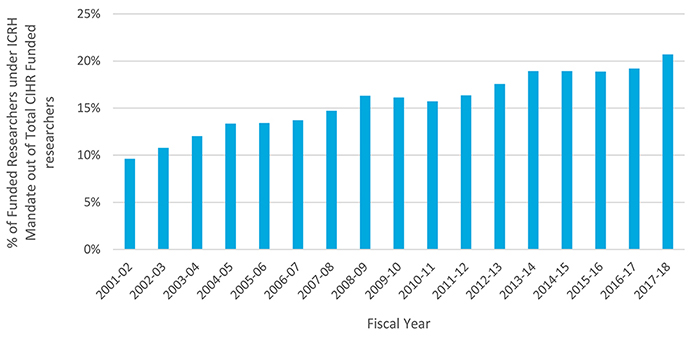
Figure 12 – Long Description
| 2000-01 | 2001-02 | 2002-03 | 2003-04 | 2004-05 | 2005-06 | 2006-07 | 2007-08 | 2008-09 | 2009-10 | 2010-11 | 2011-12 | 2012-13 | 2013-14 | 2014-15 | 2015-16 | 2016-17 | 2017-18 | Grand total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 9% | 10% | 11% | 12% | 13% | 13% | 14% | 15% | 16% | 16% | 16% | 16% | 18% | 19% | 19% | 19% | 19% | 21% | 16% |
Figure 13: Percentage of Direct Trainees Funded under IHDCYH’s Mandate
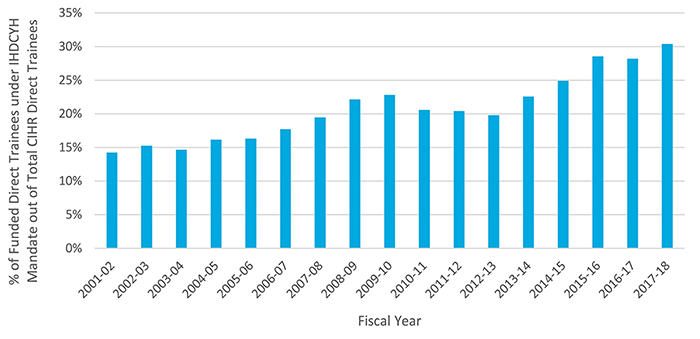
Figure 13 – Long Description
| 2000-01 | 2001-02 | 2002-03 | 2003-04 | 2004-05 | 2005-06 | 2006-07 | 2007-08 | 2008-09 | 2009-10 | 2010-11 | 2011-12 | 2012-13 | 2013-14 | 2014-15 | 2015-16 | 2016-17 | 2017-18 | Grand total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 13% | 14% | 15% | 15% | 16% | 16% | 18% | 19% | 22% | 23% | 21% | 20% | 20% | 23% | 25% | 29% | 28% | 30% | 21% |
Figure 14: Percentage of Indirect Trainees Supported under IHDCYH’s Mandate
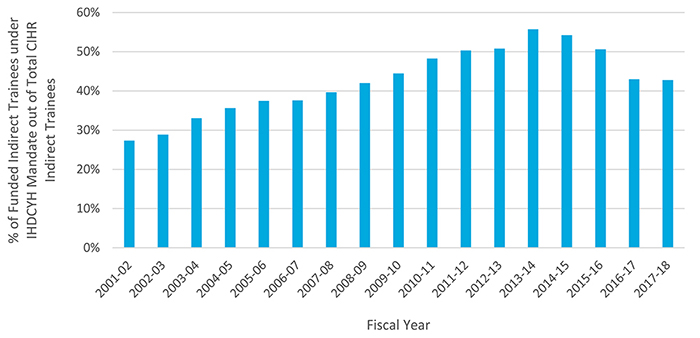
Figure 14 – Long Description
| 2001-02 | 2002-03 | 2003-04 | 2004-05 | 2005-06 | 2006-07 | 2007-08 | 2008-09 | 2009-10 | 2010-11 | 2011-12 | 2012-13 | 2013-14 | 2014-15 | 2015-16 | 2016-17 | 2017-18 | Grand total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 27% | 29% | 33% | 36% | 37% | 38% | 40% | 42% | 44% | 48% | 50% | 51% | 56% | 54% | 51% | 43% | 43% | 43% |
Figure 15: Partner Contributions to IHDCYH Funding
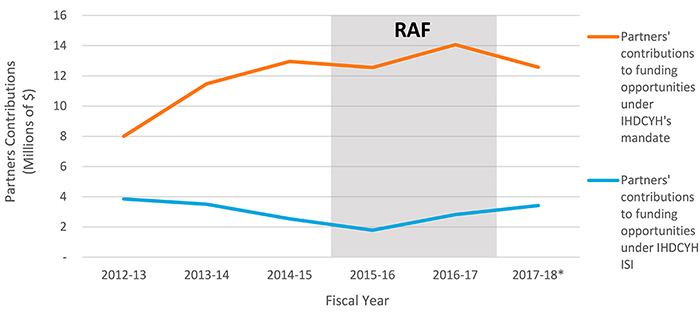
* Starting in 2017-18, Institutes regained full control of their ISI, while being required to maintain previous RAF commitments.
Figure 15 – Long Description
| Partners contributions | 2012-13 | 2013-14 | 2014-15 | 2015-16 | 2016-17 | 2017-18* |
|---|---|---|---|---|---|---|
| Partners' contributions to funding opportunities under IHDCYH's mandate | $8,005,614.00 | $11,477,182.00 | $12,954,526.00 | $12,550,872.00 | $14,064,564.00 | $12,573,517.00 |
| Partners' contributions to funding opportunities under IHDCYH ISI | $3,854,681.20 | $3,507,637.40 | $2,537,737.60 | $1,785,050.00 | $2,815,269.60 | $3,424,087.00 |
| RAF | 16000000 | 16000000 |
Figure 16: Leverage Ratio of Partnerships: Partners to Investments out of IHDCYH’s ISI Budget
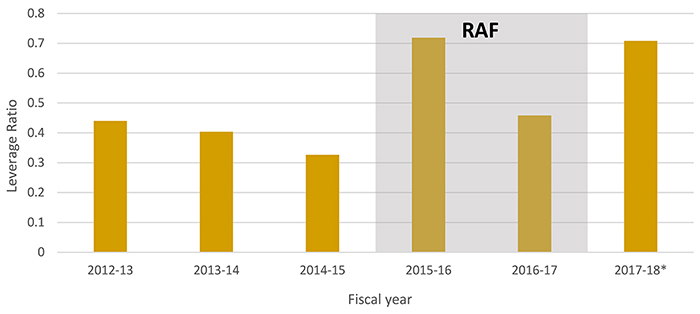
* Starting in 2017-18, Institutes regained full control of their ISI, while being required to maintain previous RAF commitments.
Figure 16 – Long Description
| 2012-13 | 2013-14 | 2014-15 | 2015-16 | 2016-17 | 2017-18* | |
|---|---|---|---|---|---|---|
| Leverage ratio | 0.440144 | 0.403633 | 0.326746 | 0.718601 | 0.458018 | 0.708255 |
| RAF | 0.8 | 0.8 |
Figure 17: Utilization of ISG Funds

Figure 17 – Long Description
| 2011-12 | 2012-13 | 2013-14 | 2014-15 | 2015-16 | 2016-17 | 2017-18 | |
|---|---|---|---|---|---|---|---|
| Institute Operations | $657,402 | $- | $724,596 | $1,007,634 | $1,022,165 | $841,563 | $753,778 |
| Institute Strategic Development | $496,336 | $- | $227,992 | $399,057 | $212,629 | $135,579 | $87,562 |
| Institute Operation and Strategic Development | $904,746 |
Figure 18: IHDCYH ISG Funding
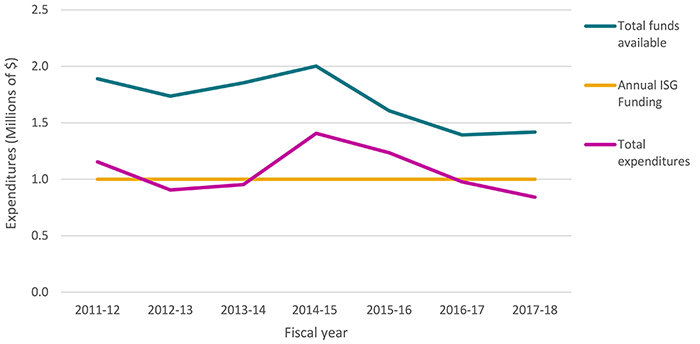
Figure 18 – Long Description
| 2011-12 | 2012-13 | 2013-14 | 2014-15 | 2015-16 | 2016-17 | 2017-18 | |
|---|---|---|---|---|---|---|---|
| Annual ISG Funding | $1,000,000 | $1,000,000 | $1,000,000 | $1,000,000 | $1,000,000 | $1,000,000 | $1,000,000 |
| Total funds available | $1,890,040 | $1,736,301 | $1,854,105 | $2,001,957 | $1,606,517 | $1,392,721 | $1,418,579 |
| Total expenditures | $1,153,738 | $904,746 | $952,588 | $1,406,691 | $1,234,794 | $977,142 | $841,340 |
| % utilization of Annual ISG Funding | 115% | 90% | 95% | 141% | 123% | 98% | 84% |
| % utilization of Total Funds Available | 61% | 52% | 51% | 70% | 77% | 70% | 59% |
- Date modified: