Institute of Circulatory & Respiratory Health – Strategic Plan 2017/18–2019/20
May 2018
Table of Contents
- Message from the Scientific Director
- Executive Summary
- About ICRH
- Objective #1
- Objective #2
- Objective #3
- Objective #4
- About CIHR
- About the ICRH Strategic Planning Process
- References
- Annex 1: ICRH Strategic Planning Advisory Committee
List of Figures
- Figure 1: Leading Causes of Death in Canada 2016
- Figure 2: Change in Proportion of ICRH Research Community Working in CIHR’s Four Themes
- Figure 3: ICRH Funding by Mandate Area (2000/01–2016/17)
- Figure 4: ICRH Network Funding
- Figure 5: Anticipated Shift in Networking Related Funding Between 2016/17–2019/20
- Figure 6: Changes in Overall Total Trainee Numbers in ICRH Mandate Areas (2007/08–2016/17)
- Figure 7: Total CIHR Funded Early Career Investigators and Total Funded in ICRH Mandate (2010/11–2015/16)
- Figure 8: ICRH Relevant Partnered Investments as a Proportion of CIHR Total Partner Investments (2009/10–2016/17)
- Figure 9: Proportion of Active ICRH Partnerships with External Partners as of February 2017
- Figure 10: Proportion of ICRH Partnerships with Various External Partners Since 2001
- Figure 11: ICRH Expenditures (2000/01–2016/17)
- Figure 12: Percentage of Projects Relevant to ICRH and Another CIHR Institute (2016/17)
- Figure 13: Rough Percentages of Citations of CIHR-Supported Cardiovascular Related Research by Continent (2008/09–2014/15)
- Figure 14: CIHR’s Action Plan on Equity
Message from the Scientific Director
The previous ICRH Strategic Plan concluded in 2017, and much has changed over the period of its mandate for the Institute. The development of this plan, in my inaugural year as Scientific Director, has provided me with the opportunity to examine the great diversity of activity undertaken by dedicated and innovative researchers across Canada, in the disciplines implicated in the circulatory and respiratory systems, including those of sleep and circadian rhythm, stroke, blood and blood vessels, and critical care. I have been impressed with the many dedicated researchers, clinicians, health service providers, and policy makers who are working to improve the health and wellness of patients and citizens in Canada; and, by extension, across the globe.
As a practicing Emergency Physician, I routinely see the impact that circulatory and respiratory disease makes on the lives of patients and families. A large percentage of patients with severe presentations seen in the emergency department are suffering from urgent repercussions of cardiovascular disease, respiratory disease, stroke, hypertension, thrombo-embolic sequelae and/or hemorrhage. Moreover, timely critical care interventions received in the acute care setting often result in patients transitioning into the inpatient and intensive care settings. Fortunately, most patients are managed and discharged; however, many patients have risk factors of future disease and an integrated primary health care system is critical for primary and secondary prevention efforts. Clearly, the research conducted within the ICRH mandate areas is critical to the health and wellness of our patients, family members, and neighbours locally, across Canada and in international communities.
The timing of our renewal consultation is opportune. In the past 15 years, the previous ICRH Scientific Directors have marshalled the ICRH community as one of the strongest in applying to CIHR’s investigator-initiated research competitions (now the Project and Foundation Grant programs). Consistently ICRH-relevant applications are proportionately amongst the top three successful mandate related topic areas, alongside genetics and cancer research (some of whose mandate specific projects address conditions such as blood cancers and genetics relevant to the ICRH mandate not considered in CIHR’s metrics). Based on past organization-wide consultations under the 2011 International Review of CIHR, ICRH was set on a course to support the development of large teams designed to address issues of knowledge creation, training and early career development, national and international collaboration, and knowledge translation. At the end of five years of funding, the ultimate goal of these networks is to be competitive in securing major funding under CIHR’s Strategy for Patient-Oriented Research (SPOR) or other Tri-Council opportunities, such as the Network Centres of Excellence (NCE) programs.
Over this same period, the nature of scientific funding in Canada and internationally has continued to evolve. A further move towards knowledge application from knowledge translation and the growth of implementation science, patient involvement in research, and the formation of multi-disciplinary, multi-pillar research necessitates that past directions be re-considered in context of current realities.
Major movements in the Government of Canada’s political direction and changes in senior leadership at CIHR underpin the incremental approach to strategic planning for ICRH. From 2014 to present, there have been unprecedented changes to CIHR, during which ICRH has worked to provide stability to the research community and support to our CIHR colleagues as we collectively work to meet the large expectations on the Institute and agency. Given ongoing work and commitments, I considered it disingenuous to launch a de novo strategic plan and potentially raise expectations that could not be met. Rather, ICRH has taken the opportunity to revisit and reflect on the past objectives, reconsidering their alignment with the direction of the Government of Canada and CIHR, and the needs of researchers, in order to reorient its three year forward looking priorities. ICRH’s Strategic Plan 2017/18–2019/20 aims to provide nimbleness in responding to new developments while continuing to position the Institute to contribute significantly to CIHR’s overarching objectives outlined in the Health Research Roadmap II, which expires in 2018/19. By looking back, acknowledging the wisdom of my predecessors and the success of our community of researchers, and looking forward in anticipation of future orientations, I believe ICRH has set a strategic plan that provides stability to our research community and which will support their evident strengths.
I am very much looking forward to working with my fellow Scientific Directors, the management team at CIHR, the many researchers within our mandate areas, as well as the excellent staff we have working at the ICRH office to meet the needs of patients, researchers and all Canadians in the prevention, detection, management and rehabilitation of circulatory and respiratory conditions.
Please join us in our efforts to deliver on this exciting vision.
Dr. Brian H. Rowe
Scientific Director
CIHR Institute of Circulatory and Respiratory Health
As a practicing Emergency Physician, I routinely see the impact that circulatory and respiratory disease makes on the lives of patients and families. A large percentage of patients with severe presentations seen in the emergency department are suffering from urgent repercussions of cardiovascular disease, respiratory disease, stroke, hypertension, thrombo-embolic sequelae and/or hemorrhage. Moreover, timely critical care interventions received in the acute care setting often result in patients transitioning into the inpatient and intensive care settings.
Executive Summary
CIHR's Institutes share responsibility for achieving the fundamental objectives of CIHR by developing strategic priorities that are aligned with the overarching directions, mandate and vision of CIHR.
The speed of discovery, convergence of disparate research fields and evolving health needs of Canadians are creating a number of significant, mutually reinforcing trends that are changing the way health research and knowledge translation are being conducted. CIHR’s Strategic Plan, Health Research Roadmap II: Capturing innovation for better health and healthcare (Roadmap II)Footnote 1 draws attention to four important areas identified by the research and stakeholder communities:
- Enhanced patient experiences and outcomes through health innovations;
- Health and wellness for Indigenous Peoples;
- A healthier future through preventive action; and
- Improved quality of life for persons living with chronic disease.
Delivering on a national health research agenda requires contributions from all members of the Canadian health research enterprise. The Institutes promote and build upon Canada's firm foundation of research excellence, engage the research community and encourage interdisciplinary, integrative health research.
Mandate and Mission
ICRH supports research into the causes, mechanisms, prevention, screening, diagnosis, treatment, support systems, and palliation for a wide range of conditions associated with the heart, lung, brain (stroke), blood, blood vessels, critical care and sleep/circadian rhythm.
This broad mandate encompasses a wide range of research communities. ICRH desires to be an active and positive contributor to the collective goals of CIHR by supporting its research community in advancing its position as a longstanding leader in addressing concerns of Canadians regarding their circulatory and respiratory health.
The ICRH Challenge
The burden of disease covered by the ICRH mandate is significant. Circulatory and respiratory disease (including stroke) continues to be a major source of morbidity and mortality, costing the Canadian economy in terms of public and private health care costs and lost productivity. Reflecting on this, the ICRH research community has advanced the science and knowledge uptake to help address these concerns; however, new risks are emerging. Lifestyle habits with respect to smoking, diet, and exercise and environmental influences are contributing to increased risk factors for many diseases within the ICRH mandate areas. Hypertension, diabetes, and obesity are on the rise and pose additional threats to the impressive health and wellness improvements achieved over the past half century in Canada.
ICRH also has responsibility to grow capacity in the smaller research communities within its mandate. The importance that sleep/circadian rhythm and critical care play in maintaining health cannot be overlooked, nor set aside. Finding a balance in supporting such varied communities is at the core of ICRH’s work.
Figure 1: Leading Causes of Death in Canada 2016
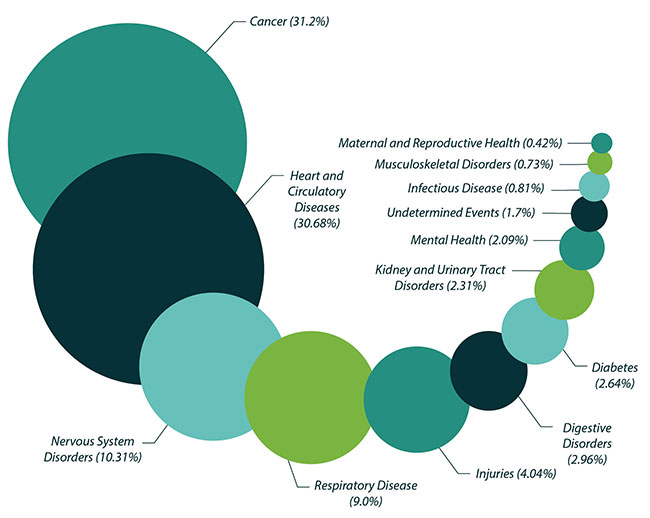
Institute for Health Metrics and Evaluation (IHME). GBD Compare Data Visualization. Seattle, WA: IHME, University of Washington. (Accessed December 21, 2017)
Figure 1 long description
| Cause | Percentage of total deaths |
|---|---|
| Cancer | 31.2% |
| Heart and Circulatory Diseases | 30.68% |
| Nervous System Disorders | 10.31% |
| Respiratory Disease | 9.0% |
| Injuries | 4.04% |
| Digestive Disorders | 2.96% |
| Diabetes | 2.64% |
| Kidney and Urinary Tract Disorders | 2.31% |
| Mental Health | 2.09% |
| Undetermined Events | 1.7% |
| Infectious Disease | 0.81% |
| Musculoskeletal Health | 0.73% |
| Maternal and Reproductive Health | 0.42% |
Refreshed Strategic Plan
Perhaps more so than any other of CIHR’s Institutes, ICRH has focused, over the past strategic planning cycle, on coalescing researchers across its mandate areas into large teams and networks. This strategy is demonstrating value by mobilizing national leaders, researchers, and partners to solve complex research questions and support the development of a strong pipeline of new, diverse and skilled researchers across the four CIHR research themesFootnote 2. These investments have, however, created additional challenges to providing a comprehensive program of supports to our research community until these funding commitments end, their impact is evaluated, and their contribution to reaching past objectives discerned. Only at that time will it be reasonable to set ICRH on a new course of action.
With these considerations in mind, ICRH consulted with its community leaders to refresh its priorities and identify objectives to be reached over a shorter timeframe. It also worked to gather information directly from the research community that identifies with the ICRH mandate, either self-identified or identified directly through receipt of ICRH funding.
From these activities, ICRH has renewed a commitment to work towards fulfilling the following research priorities in order to meet several objectives.
Research Priorities
Working collaboratively with diverse partners to increase the resources and opportunities for research funding within its mandate areas, ICRH plans to:
- Facilitate networking within, and among ICRH’s research community and to other stakeholders in the research enterprise nationally and internationally;
- Enhance training and early career development to build future research and knowledge leaders within ICRH mandate areas;
- Enhance the conduct of Indigenous Health Research and equitable research under ICRH’s mandate areas; and
- Enhance the ICRH research community’s ability to participate in and contribute to the multi-Institute signature initiatives launched collectively by Science Council.
Institute Objectives
In the next three years ICRH expects to see that:
- Resources and opportunities are increased through collective effort for training and early career development in the ICRH community;
- Stakeholders and partners are engaged and perceive ICRH as able to facilitate their participation in the Institute’s activities;
- Researchers working in ICRH mandate areas are further represented in national and international research and knowledge translation and implementation activities; and
- Health and health system impacts are realized from research conducted in the ICRH mandate areas, particularly for Canada’s Indigenous Peoples (First Nations, Inuit and Métis) and populations facing potential systematic biases.
About ICRH
Along with the other Institutes, ICRH shares responsibility for achieving the fundamental objectives of CIHR by developing strategic priorities that are aligned with the overarching directions, mandate and vision of CIHR. Health Research Roadmap II: Capturing innovation for better health and healthcare (Roadmap II) sets out CIHR’s strategic directions to 2018/19.
The Institute represents a large community of researchers working across CIHR’s four themes and historically has a larger constituency of biomedical (Theme/Pillar I) and clinical (Theme/Pillar II) researchers than CIHR as a whole. Reflecting CIHR’s dual mandate to generate new knowledge and move that knowledge into practice, the community of researchers within the ICRH mandate working in health services, policy (Theme/Pillar III) as well as population and public health (Theme/Pillar IV) has been slowly growing.
Figure 2: Change in Proportion of ICRH Research Community Working in CIHR’s Four Themes
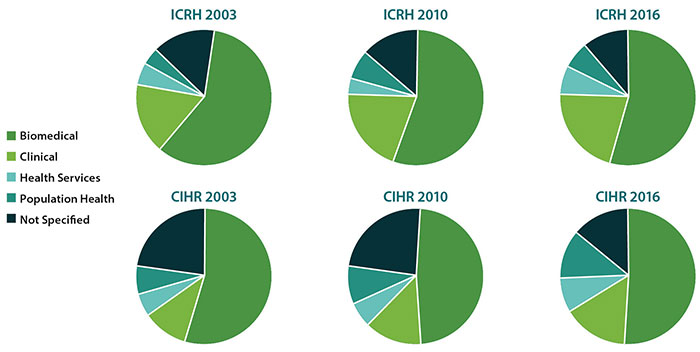
Figure 2 long description
| CIHR Research Theme | 2003 | 2010 | 2016 |
|---|---|---|---|
| Biomedical | 61.4% | 56.0% | 54.2% |
| Clinical | 17.0% | 20.0% | 21.7% |
| Health Services | 5.0% | 3.6% | 6.5% |
| Population Health | 4.1% | 7.0% | 6.5% |
| Not Specified | 12.5% | 13.5% | 11.0% |
| CIHR Research Theme | 2003 | 2010 | 2016 |
|---|---|---|---|
| Biomedical | 54.7% | 49.1% | 51.0% |
| Clinical | 10.7% | 13.4% | 15.5% |
| Health Services | 5.0% | 6.0% | 8.1% |
| Population Health | 7.3% | 9.5% | 11.8% |
| Not Specified | 22.3% | 22.0% | 13.6% |
ICRH Mandate
The mandate of the Institute of Circulatory and Respiratory Health (ICRH) is to support research into the causes, mechanisms, prevention, screening, diagnosis, treatment, support systems, and palliation for a wide range of conditions associated with the heart, lung, brain (stroke), blood, blood vessels, critical care and sleep/circadian rhythm.
ICRH Mission
The broad ICRH mandate encompasses a wide range of research communities. ICRH looks to be an active and positive contributor to the collective goals of CIHR by supporting its research community in advancing its position as a longstanding leader addressing concerns of Canadians regarding their circulatory and respiratory health.
The ICRH Challenge
The burden of disease covered by the ICRH mandate is significant. Circulatory and respiratory disease (including stroke) continues to be a major source of morbidity and mortality, costing the Canadian economy in terms of public and private health care costs and lost productivity. Reflecting this, the ICRH research community has advanced the science and knowledge uptake to help address these concerns; however, new risks are emerging. In many of the ICRH mandate areas, Canadian researchers are international research and thought leaders; despite Canada’s smaller academic community, these researchers are making major discoveries that are changing the face of health and wellness locally, nationally and internationally.
While research advancement has been impressive, much work remains. The prevalence rates for chronic cardiovascular and respiratory diseases have increased since 2000, reflecting that more Canadians are living with those diseases every year. In 2011/12, an estimated 2.3 million Canadians were living with ischemic heart disease, almost 2 million were living with chronic obstructive pulmonary disease (COPD), and approximately 700,000 were living with the effects of a strokeFootnote 3.
Demographics, environmental threats and lifestyle habits with respect to smoking, diet, and exercise and environmental influences are now contributing to increased risks for many diseases within the ICRH mandate areas. Hypertension, diabetes, and obesity are on the rise and pose additional threats to the impressive health and wellness improvements achieved over the past half century in Canada. The lifetime risk for developing hypertension among adults aged 55 to 65 years with normal blood pressure is 90%. Hypertension is the most common reason to visit a doctor; the number one reason for taking medication; and significantly increases risk for stroke, ischemic heart disease, peripheral vascular disease and heart failure. More than one in five Canadian adults aged 20 years and older are living with diagnosed hypertension, while an estimated 17% are not aware they have the conditionFootnote 4.
ICRH also has responsibility to grow capacity in the smaller research communities within its mandate. The importance that sleep/circadian rhythm and critical care play in maintaining health cannot be overlooked nor set aside. People with untreated obstructive sleep apnea have an increased risk of motor vehicle crashes, cardiovascular disease, hypertension and early death. Finding a balance in supporting such varied communities is at the core of ICRH’s work. Outbreaks of pandemic diseases (e.g., Severe Acute Respiratory Syndrome (SARS), H1N1 Influenza and Ebola), responses to natural disasters (e.g., wildfires, floods, ice storms and tornados), and the increasing threat from bio-terrorism underscore the need for building research capacity in the delivery of critical care and disaster preparedness.
ICRH Investments
Annually, ICRH has $8.6M at its disposal for research investments that are priority-driven to build and support strategic research targeting our mandate areas. This is in addition to CIHR grants and awards provided through the Project and Foundation Grant programs that support investigator-initiated proposals in the ICRH mandate areas. In any year, only a percentage of ICRH’s strategic budget is available for new investment, as funding given in prior years can have multi-year payment terms that are honored over time.
Following the 2011 International Review, CIHR and ICRH in particular placed increased emphasis on developing formal research networks. The International Review Panel Report noted Institutes’ success in transforming the research environment by acting as a catalyst, convener, and creator of networks and partnerships, and encouraged further collaboration across research themes. It recommended the establishment of centres of excellence which would function as collaborative networks for the training of future clinical and translational researchers, particularly first-in-man studies where a new concept developed in the test tube and animal models is first tested in humans (T1 knowledge transfer) and knowledge transfer into the delivery of care; and, where appropriate, commercialization (T2 knowledge transfer).
CIHR operationalized this approach through many programs, as exemplified by the Strategy for Patient-Oriented Research (SPOR). Under Strategic Plan 2013–2016, ICRH responded to a direct recommendation to see that networking “forms the central plank of the new quinquenium” by investing heavily in clinical research. Through a series of competitions, ICRH funded three Emerging Networks, five Community Development Program teams, and three large teams linked to CIHR Signature Initiatives.
Figure 3: ICRH Funding by Mandate Area (2000/01 – 2016/17)
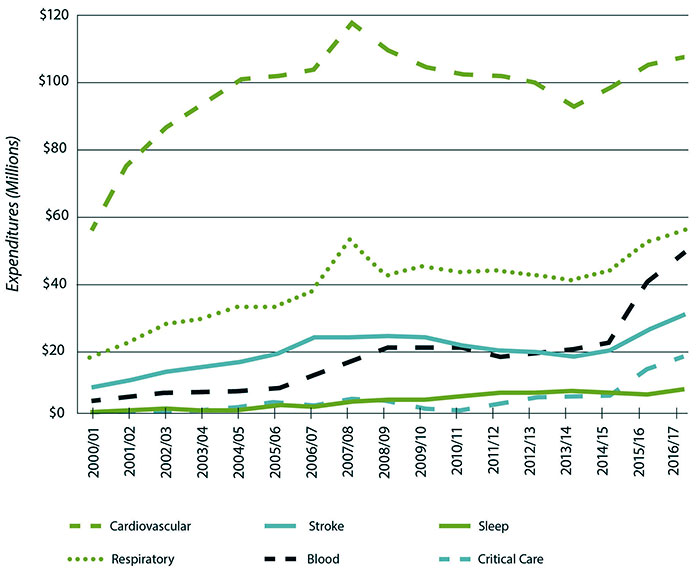
Figure 3 long description
| Year | Cardiovascular | Respiratory | Stroke | Blood | Sleep | Critical Care |
|---|---|---|---|---|---|---|
| 2000/01 | $55,561,280.33 | $16,214,354.28 | $7,378,284.81 | $3,038,997.66 | $416,400.50 | $0 |
| 2001/02 | $74,362,306.18 | $21,249,712.54 | $9,813,734.81 | $4,535,219.12 | $605,266.33 | $167,516.00 |
| 2002/03 | $86,787,685.98 | $27,080,783.56 | $12,480,075.47 | $6,019,847.31 | $580,943.00 | $592,860.00 |
| 2003/04 | $93,680,845.90 | $28,483,152.66 | $13,662,846.98 | $6,326,072.67 | $848,033.00 | $678,725.00 |
| 2004/05 | $100,500,399.67 | $31,649,286.36 | $15,611,380.38 | $6,525,125.00 | $945,071.00 | $1,179,196.00 |
| 2005/06 | $101,894,323.13 | $31,949,809.97 | $17,917,498.80 | $7,522,377.57 | $1,707,660.00 | $1,932,049.00 |
| 2006/07 | $103,966,314.14 | $36,392,448.05 | $22,282,881.67 | $10,462,866.46 | $1,825,100.58 | $1,361,549.00 |
| 2007/08 | $117,733,033.04 | $51,050,313.34 | $22,157,890.05 | $14,915,666.79 | $2,475,418.00 | $2,711,920.00 |
| 2008/09 | $109,025,691.49 | $41,341,330.36 | $23,009,455.67 | $19,528,985.54 | $2,537,751.48 | $2,843,492.00 |
| 2009/10 | $104,417,106.69 | $43,602,270.88 | $22,294,436.67 | $20,095,419.96 | $3,217,504.50 | $1,063,362.00 |
| 2010/11 | $102,329,647.22 | $41,626,016.31 | $19,831,406.30 | $20,125,205.82 | $4,638,202.00 | $872,365.00 |
| 2011/12 | $101,045,045.73 | $42,284,419.86 | $18,489,528.57 | $16,906,322.00 | $5,323,772.00 | $2,278,711.00 |
| 2012/13 | $99,205,311.10 | $41,236,877.52 | $18,074,345.67 | $17,330,759.00 | $5,333,963.00 | $3,977,019.00 |
| 2013/14 | $93,288,376.67 | $40,419,243.00 | $15,971,603.00 | $18,849,831.00 | $5,392,891.00 | $4,093,610.00 |
| 2014/15 | $98,025,721.99 | $42,103,022.00 | $19,329,827.00 | $20,732,705.00 | $5,755,240.00 | $4,994,737.00 |
| 2015/16 | $104,984,450.00 | $51,112,495.21 | $25,117,087.00 | $39,103,424.00 | $5,253,684.00 | $13,135,555.00 |
| 2016/17 | $107,856,186.00 | $55,167,461.00 | $29,281,928.00 | $48,175,434.00 | $6,117,575.00 | $18,498,124.00 |
A change in the CIHR financial framework enacted in 2014, however, sets expectations for all CIHR Institutes to strategically target 50% of its resources toward large scale priority-driven research programs that meet the objectives of multiple Institutes. Under this directive, ICRH’s investments supporting networking must move from a mandate-specific emphasis towards efforts to support networking that reaches broader objectives for CIHR’s Institutes collectively.
Strategic Plan 2017/18–2019/20 establishes a forward looking vision for transitioning the network connections of ICRH’s research community towards an approach needed to reach beyond Canada’s community of health researchers and transcends traditional ways of working. Including stakeholders and knowledge users, pooling resources and taking collective action on complex challenges is requisite for the health research enterprise’s accelerated and long-term success.
Figure 4: ICRH Network Funding

Figure 4 long description
| Funded Network | Years |
|---|---|
| International Collaboration | 2013-2018 |
| ICRH Sponsored Signature Initiative large teams | 2013-2018 |
| ICRH Emerging Networks | 2013-2018 |
| ICRH Community Development Program large teams | 2014-2019 |
| ICRH Community Development Program large teams | 2015-2020 |
| ICRH Sponsored Signature Initiative large teams | 2016-2021 |
Figure 5: Anticipated Shift in Network Related Funding Between 2016/17-2019/20
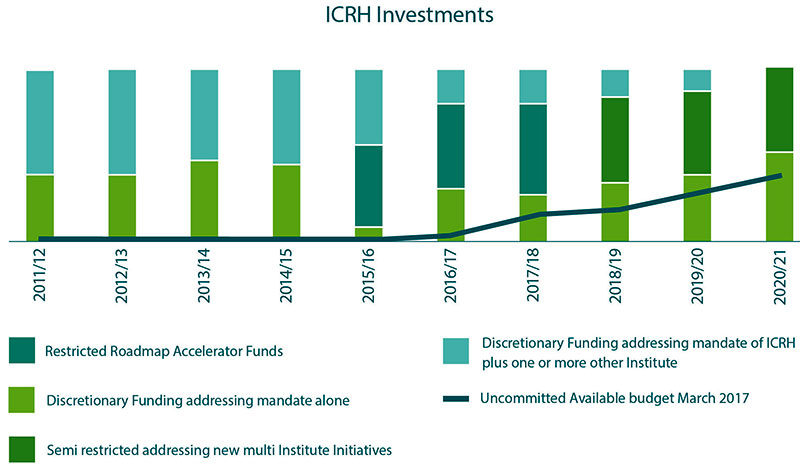
Figure 5 long description
| 2011/12 | 2012/13 | 2013/14 | 2014/15 | 2015/16 | 2016/17 | 2017/18 | 2018/19 | 2019/20 | 2020/21 | |
|---|---|---|---|---|---|---|---|---|---|---|
| Discretionary funding addressing mandate of ICRH plus one or more other Institute | $5.2M | $5.3M | $4.5M | $4.7M | $3.9M | $1.7M | $1.7M | $1.4M | $1.0M | $0 |
| Semi restricted addressing new multi Institute initiatives | $0 | $0 | $0 | $0 | $0 | $0 | $0 | $4.3M | $4.3M | $4.3M |
| Restricted Roadmap Accelerator Funds | $0 | $0 | $0 | $0 | $4.3M | $4.3M | $4.3M | $0 | $0 | $0 |
| Discretionary funding addressing ICRH mandate alone | $3.4M | $3.3M | $4.1M | $3.9M | $0.4M | $2.6M | $2.6M | $2.9M | $3.3M | $4.3M |
| Uncommitted Available budget March 2017 | $0 | $0 | $0 | $0 | $0 | $0.2M | $1.2M | $1.5M | $2.4M | $3.4M |
Research Priorities 2017/18–2019/20
Working collaboratively with diverse partners to increase the resources and opportunities for research funding within its mandate areas, ICRH plans to:
- Facilitate networking within, and among ICRH’s research community and to other stakeholders in the research enterprise nationally and internationally;
- Enhance training and early career development to build future research and knowledge leaders within ICRH mandate areas;
- Enhance the conduct of Indigenous Health Research and equitable research under ICRH’s mandate areas; and
- Enhance the ICRH research community’s ability to participate in and contribute to the multi-Institute signature initiatives launched collectively by Science Council.
ICRH has set several objectives by which it plans to address these four priorities over the term of this strategic plan. These are outlined in the following pages.
Objective #1
Training and early career development is an important focus for CIHR and its Institutes. Creating a robust, inclusive and enriching environment that supports the researchers of tomorrow is a priority of the health research enterprise. Traditionally, undergraduate, graduate and post-graduate research and clinician-scientist trainees within the ICRH mandate areas have received consistent CIHR support and achieved remarkable success. Recent monitoring suggests that this support has decreased and the ICRH strategic refresh emphasizes an ongoing commitment to training and career development within its mandate, which is necessary to regain momentum.
The ICRH community has seen a steady decline of Postdoctoral Fellowships awarded over the last decade (>50%), and a 50% drop in Doctoral Studentships that mirrors an overall drop in CIHR Doctoral Studentships in the last 5 years. A doubling of the number of ICRH relevant Master’s Studentships in the last two years has done little to mitigate against a 40% decrease in total trainee awards in the ICRH mandate areas. The concerning trends seen for trainees in the ICRH mandate areas mirrors an overall drop in all CIHR trainee awards in the past 5 years.
ICRH has also observed an approximate 50% drop in doctoral and fellowship awards in the cardiovascular and respiratory mandate areas in the last 5 to 10 years; mandate areas that have traditionally been very successful at attracting trainees into their research programs. Moreover, while an increase in Master’s Studentships in the blood and sleep mandate areas was observed, the relative size of these communities have historically been small when compared to the cardiovascular and respiratory mandate areas. As such, any increase in trainees seen within the sleep and blood mandate areas have had little effect on the total number of trainees supported within the ICRH mandate over the last decade.
Figure 6: Changes in Overall Total Trainee Numbers in ICRH Mandate Areas (2007/08-2016/17)
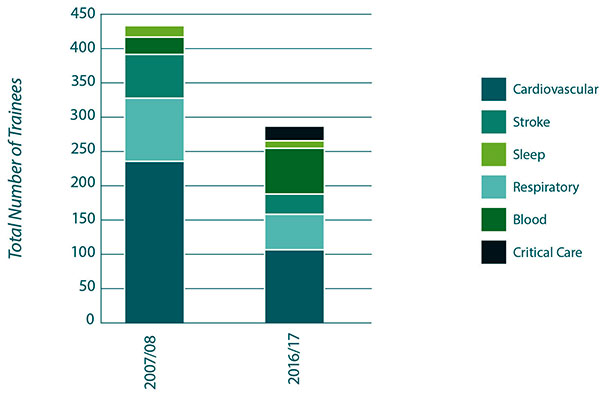
Figure 6 long description
| Mandate Area | 2007/08 | 2016/17 |
|---|---|---|
| Cardiovascular | 242 | 108 |
| Respiratory | 90 | 53 |
| Stroke | 67 | 30 |
| Blood | 27 | 64 |
| Sleep | 10 | 13 |
| Critical Care | 0 | 22 |
As we reflect on the burden of disease covered by the ICRH mandate, these are concerning statistics. The health and wellness of Canadians depends on having a diverse, dynamic, and highly-qualified work force. This requires engaged leaders and experts across the Canadian health research enterprise with the skills and confidence necessary to undertake major health challenges facing us, and innovate in the knowledge economy. Ensuring the quality and relevance of health research training to attract young people is critical to building a solid foundation for the future, and to better position trainees for success and impact. To this end, CIHR has developed a Strategic Action Plan on Training which identifies priorities toFootnote 5:
- Create research leaders of tomorrow by developing individuals who can lead high-impact, multi-disciplinary research in a rapidly evolving environment of advancing technologies and globalization;
- Create leaders across knowledge sectors by developing individuals who can apply their scholarship and talent to lead innovation across different sectors of Canada’s knowledge-based economy; and,
- Create experts in critical priority areas by developing individuals who can establish and fill Canadian priority areas of specialized expertise and advance the frontiers of science.
In support of this, ICRH has developed a framework to guide the training and early career development activities for the Institute. The framework focuses on graduate students, postgraduate fellows and new investigators (within the first 60 months of first academic appointment) across the four research pillars and ICRH mandate areas as the primary targets for training and early career development. High school and undergraduate students are recognized as important inputs to the training and early career development framework; however, they are not specifically identified in the current framework as they are considered to be in a phase of exposure to a wide range of potential career interests which is yet to become sufficiently focused for attention. Targeted training and early career development activities included in the framework are core competencies and career development training. Core competencies are defined under four broad categories as follows: technical skills; professional skills; mentorship; and, leadership. Career development activities range from career exploration, to career specialization and finally career achievement.
Figure 7: Total CIHR Funded Early Career Investigators and total funded in ICRH Mandate (2010/11-2015/16)
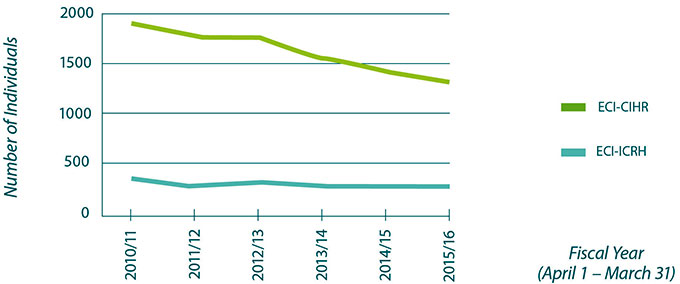
*Data based on grants funded up to CIHR fiscal year 2015/16, a general Grants and Awards (G&A) dataset updated until 28 June 2017, and an All Persons dataset updated until 20 April 2017.
Figure 7 long description
| 2010/11 | 2011/12 | 2012/13 | 2013/14 | 2014/15 | 2015/16 | |
|---|---|---|---|---|---|---|
| ICRH | 303 | 253 | 312 | 273 | 246 | 244 |
| CIHR | 1859 | 1732 | 1703 | 1552 | 1433 | 1336 |
ICRH continues to be active in supporting Early Career Investigators (ECIs) through development of funding opportunities targeted specifically to researchers at this stage in their career. The critical move to an independent research career is recognized as a difficult step, and one that can derail interested clinicians from continuing to pursue a research career. This strategy is showing signs of promise with ECIs in the ICRH mandate accounting for roughly 17% of total number of CIHR supported ECIs. Simultaneously there has been relatively consistent support of ECIs within the ICRH mandate areas against an overall 30% decrease in CIHR funded ECIs in the past 5 years. The pattern of shifting expertise, however, continues with the observed number of cardiovascular focused ECIs decreasing.
ICRH will continue to focus efforts on re-connecting trainees across the career stages to the ICRH mandate by executing activities that support their development. This is accomplished in collaboration with our partners and stakeholders to ensure opportunities are value added to both sponsors and trainees. For example, ICRH partners on the training and career development programs at major Society meetings in cardiovascular (Canadian Cardiovascular Society {CCS}), respiratory (Canadian Respiratory Conference {CRC}), critical care (Canadian Critical Care Forum {CCCF}), sleep (Canadian Sleep Society {CSS}) and other related mandate areas. An important contribution to this mandate arises from the activities of the Emerging Networks and Community Development Programs, where important mentorship and training opportunities are encouraged and created.
Building Capacity for Tomorrow
ICRH’s Commitment to Trainees
While the research environment in Canada is always evolving, the need to support the next generation of research trainees remains a constant. ICRH recognizes the need to provide critical support for national trainee workshops within the Institute’s mandate areas. Working in collaboration with various partners, ICRH will provide continued support for events and workshops like the Lung Association’s RENASCENT/CIHR-ICRH Training Workshop and the CCS/CIHR-ICRH Annual Cardiovascular Trainee Day hosted as part of the Canadian Cardiovascular Congress. These workshops provide trainees with the opportunity to build technical and professional skills, engage in leadership opportunities and interact with leading Canadian researchers in a mentorship capacity.
ICRH’s Commitment to Early Career Investigators
Early Career Investigators (ECIs) are defined by CIHR as researchers within the first 60 months of their first academic appointment. ICRH understands the critical need to support Canadian researchers during the initial years of independent investigation. Through initiatives like the ECI Awards in Circulatory and Respiratory Health and the ECI in Maternal, Reproductive, Child and Youth Health, the Institute provides funding and protected research time to ECIs in Canada. These important awards will continue to be a implemented as a key piece of the ICRH’s commitment to ECIs.
Objective #2
CIHR, as a federal organization, has the ability to marshal resources, lead on policy issues and address strategic areas of research that require support, are of high social value, and at times may be relatively unaddressed; however, it is only one participant in a complex system of research funders. Other stakeholders include Academic Institutions, Industry, Not-for-Profit organizations and Societies, Research Networks, Trainee Groups, other Federal/Provincial and Territorial Governmental Organizations, and other Research Funding Organizations. For ICRH in particular, stakeholders have played a large and important role in the past and we anticipate that the need for these partnerships will only increase in the future.
Organizations such as The Heart & Stroke, The Lung Association, Hypertension Canada and Thrombosis Canada provide critical support to research that has a positive impact on Canadian lives. More than nine percent of clinical trials run in Canada by innovative pharmaceutical and biologic companies are focused on cardiovascular diseaseFootnote 6.
Alongside ICRH, a number of stakeholder groups share the role and responsibility for delivering training on core competencies and career development, depending on their development priorities, needs, respective objectives, and anticipated outcomes.
Relatively speaking, partner investments in research relevant to the ICRH mandate is significant, and much higher than might be anticipated given the existence of twelve other Institutes.
While the cardiovascular, stroke, blood and blood vessels and respiratory research communities have well-established supporters, other communities in the ICRH mandate areas are not so fortunate. The critical care and sleep/circadian rhythm communities do not have such natural alignment for partnership supports, other than that which exists within the health care and, to a lesser extent, education systems.
Figure 8: ICRH Relevant Partnered Investments as a Proportion of CIHR Total Partner Investments (2009/10-2016/17)
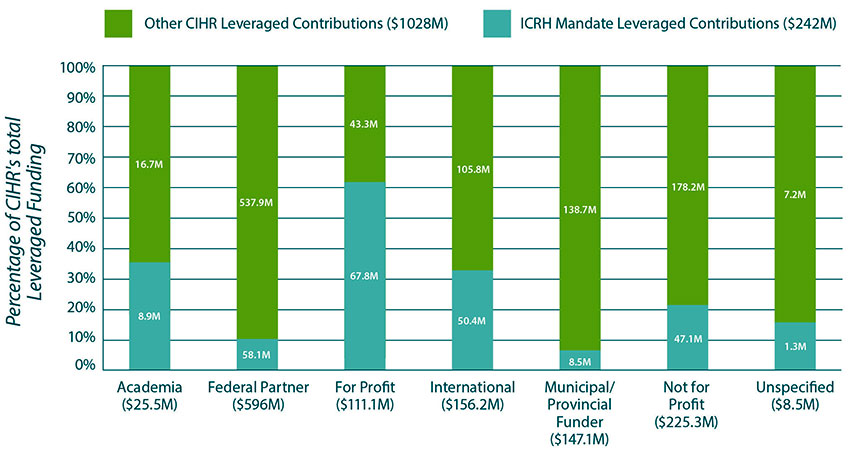
Figure 8 long description
| Other CIHR Leveraged Contributions | ICRH Mandate Leveraged Contributions | Total | |
|---|---|---|---|
| Academia | $16.7M | $8.9M | $25.5M |
| Federal Partner | $537.9M | $58.1M | $596M |
| For Profit | $43.3M | $67.8M | $111.1M |
| International | $105.8M | $50.4M | $156.2M |
| Municipal/Provincial Funder | $138.7M | $8.5M | $147.1M |
| Not for Profit | $178.2M | $47.1M | $225.3M |
| Unspecified | $7.2M | $1.3M | $8.5M |
| Total | $1028M | $242M | $1270M |
The funding of the ICRH Emerging Networks and Community Development Program teams were contingent on the commitment of partners to the objectives of their programs of research. It is clear from these activities that there is much common ground of interest. Teams reached close to dollar-for-dollar commitments in partner funding against that of ICRH at application and continue to demonstrate high levels of partnership funding.
ICRH is committed to working with its established and emerging partners so that it can maximize collaboration to meet our collective interest, and to seeking out and cultivating new and novel relationships to provide support to expanding communities of its researchers. Since the inception of CIHR, ICRH has partnered with nineteen different organizations and groups on over 60 different initiatives. In February 2017, ICRH had 12 active initiatives and four new initiatives under discussion with 10 different organizations. The following Figures provide a historic and recent breakdown, respectively, of the proportion of partnerships with charitable groups, international groups, industry, professional organizations, external research groups and government partners.
ICRH strongly believes that CIHR funding is a mark of scientific quality, merit and integrity that partners can trust in maximizing the potential success of their committed resources to a particular course of action. The ICRH team also firmly believes that more can be achieved if we work with partners to meet collective goals. In an environment of flat or constricting research budgets and increasing competitiveness it is even more important that we work with stakeholders to see our collective resources applied to the greatest expected outcomes. We will continue to build strong and effective relationships to see that our collective investments are put to innovative research, effective knowledge translation and implementation; ultimately providing maximum benefit to the health and wellness of Canadians.
Figure 9: Proportion of Active ICRH Partnerships with External Partners as of February 2017
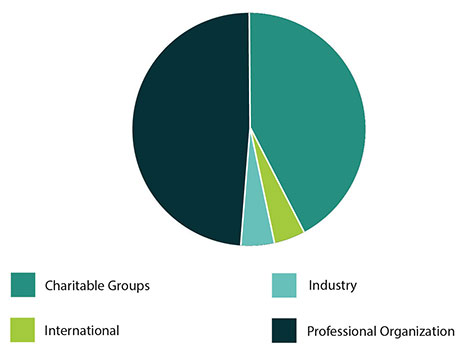
Figure 9 long description
| External Partner Type | Number of Active Partnerships |
|---|---|
| Professional Organizations | 10 |
| Charitable Groups | 9 |
| International | 1 |
| Industry | 1 |
Figure 10: Proportion of ICRH Partnerships with Various External Partners Since 2001
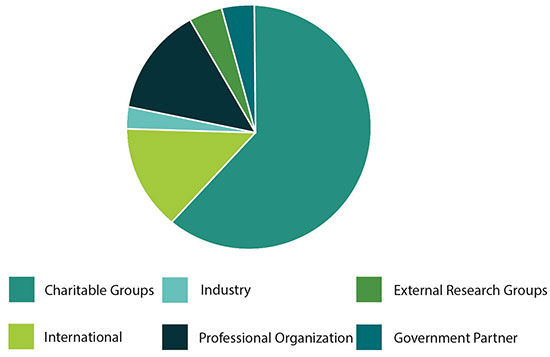
Figure 10 long description
| External Partner Type | Number of Partnerships |
|---|---|
| Charitable Groups | 37 |
| Professional Organizations | 10 |
| International | 9 |
| Industry | 2 |
| External Research Groups | 2 |
| Government Partners | 2 |
Celebrating Excellence
Distinguished Lecturer Award Series
The ICRH Distinguished Lecturer Award Series (DLA) recognizes and honours outstanding investigators from each ICRH mandate area who have contributed significantly to the advancement of science in their field of research both in Canada and internationally. In collaboration with partners which include the Canadian Cardiovascular Society, the Canada Critical Care Society, the Canadian Thoracic Society, the Canadian Sleep Society and the Canadian Society of Atherosclerosis, Thrombosis and Vascular Biology, the DLA facilitates knowledge translation through keynote lectureships at national conferences. These partnerships provide an opportunity to engage with the ICRH scientific community and recognize research excellence in Canada.
Lasting Partnerships
Chair in Hypertension Prevention and Control
Since 2006, ICRH has supported a Chair in Hypertension Prevention and Control, an award that expanded in 2010 to include partnerships with The Heart & Stroke and Hypertension Canada. The first recipient was Dr. Norman Campbell, an accomplished clinician-scientist from the University of Calgary. Dr. Campbell is a General Internist, a Professor of Medicine, Community Health Sciences and Physiology and Pharmacology and a member of the O’Brien Institute of Public Health and Libin Cardiovascular Institute of Alberta at the University of Calgary.
The $1.125 million award was re-launched in 2016 and awarded to Dr. Janusz Kaczorowski, Professor, Research Director and Principal Scientist at the University of Montreal Hospital Research Centre. Over the next five years, Dr. Kaczorowski will continue to pursue research that supports the development of novel system-wide strategies, which translate to improved blood pressure control and prevention of hypertension and associated chronic diseases among Canadians.
Objective #3
As one can surmise, ICRH’s mandate overlaps with those of a number of other CIHR Institutes and collaboration among Institutes has been one of the hallmarks of the CIHR organizational structure. Grants and awards that are relevant to the ICRH mandate are often also relevant to one or more of the other Institutes’ mandates. Most significantly, ICRH's mandate overlaps quite closely with those of the Institute of Gender Health, the Institute of Infection and Immunity, the Institute of Genetics, the Institute of Nutrition, Metabolism and Diabetes, the Institute of Human Development Child and Youth Health, the Institute of Neurosciences, Mental Health and Addiction and the Institute of Health Services and Policy Research (in descending order). The following are examples of types of research topics which have significant crossover between an ICRH sub-mandate area and those of other Institutes:
- Respiratory: Immunity, childhood diseases, public health tobacco cessation interventions;
- Blood: immunity (i.e., regenerative medicine, stem cells), cancer;
- Stroke: Neuroscience, dementia management, physical rehabilitation, long-term care;
- Cardiovascular: Differential health outcomes (e.g., for gender diverse and Indigenous Peoples), health system integration, diabetes management, public health prevention interventions;
- Critical Care: Infection/sepsis, musculoskeletal and workplace injuries, care for the aged; and
- Sleep/Circadian Rhythm: Cognitive function, changes from aging, nutrition and obesity.
In order to avoid significant double counting of research across Institutes, ICRH does not generally report on research projects not directly related to an impact on circulatory or respiratory health (e.g., blood and lung cancers, the immunological actions of blood cells or genetics projects relating to the tissues of the heart, lung, bone marrow etc.), except in the case where no other Institute’s mandate is likely to incorporate them. While these projects are considered of true relevance to Canadians' health, and the major components of the cardiopulmonary system, they are counted in the metrics of other Institutes.
As noted in the expenditures by Institute mandate areas, there has been little apparent growth in granting under the ICRH mandate in the past decade; however, this reporting does not effectively capture the multi-disciplinary environment in which today’s researchers work.
Bibliometric evidence indicates that the ICRH research community continues to contribute significantly to the world literature in cardiovascular research. Figure 13 shows approximate percentages of citations of CIHR-supported cardiovascular related research by continent between 2008 and 2014. With increased collaboration of the CIHR Institute mandates we anticipate that this knowledge mobility will be further increased. Recent analysis of international collaboration in cardiovascular research shows that research findings have higher impact when research is conducted by teams having cross-border collaborations behind themFootnote 7.
Figure 11: ICRH Expenditures (2000/01-2016/17)

Figure 11 long description
| Year | ICRH Expenditures |
|---|---|
| 2000/01 | $76,243,638.64 |
| 2001/02 | $102,118,664.85 |
| 2002/03 | $121,983,954.55 |
| 2003/04 | $130,949,429.23 |
| 2004/05 | $140,852,651.03 |
| 2005/06 | $145,198,964.67 |
| 2006/07 | $154,453,964.65 |
| 2007/08 | $178,642,420.17 |
| 2008/09 | $175,791,363.37 |
| 2009/10 | $175,573,279.03 |
| 2010/11 | $173,967,441.35 |
| 2011/12 | $170,843,641.59 |
| 2012/13 | $166,584,399.62 |
| 2013/14 | $156,991,789.67 |
| 2014/15 | $158,564,244.99 |
| 2015/16 | $167,040,873.21 |
| 2016/17 | $174,610,904.00 |
Figure 12: Percentage of Projects Relevant to ICRH an Another CIRH Institute (2016/17)
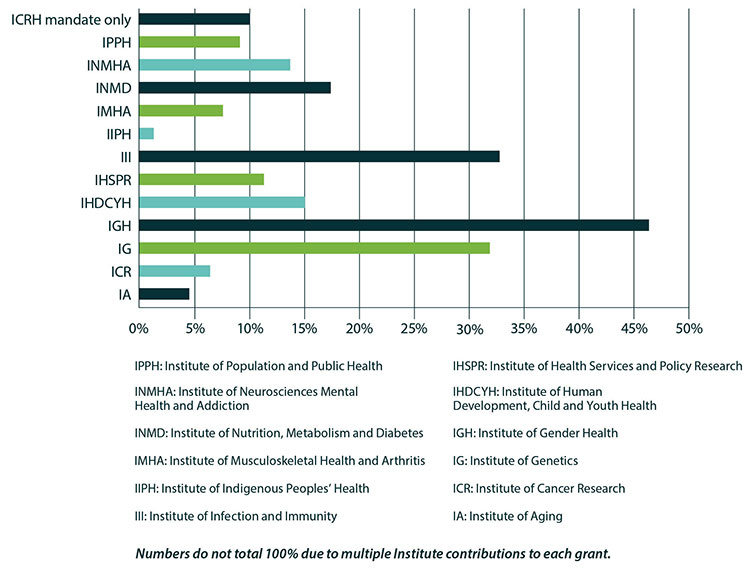
Figure 12 long description
| Institute | % of Total Number of Unique Projects Relevant to ICRH |
|---|---|
| ICRH Mandate Only | 10.0 |
| Institute of Population and Public Health | 9.2 |
| Institute of Neurosciences Mental Health and Addiction | 13.8 |
| Institute of Nutrition, Metabolism and Diabetes | 17.7 |
| Institute of Musculoskeletal Health and Arthritis | 7.4 |
| Institute of Indigenous Peoples’ Health | 1.2 |
| Institute of Infection and Immunity | 32.9 |
| Institute of Health Services Policy Research | 10.9 |
| Institute of Human Development, Child and Youth Health | 15.1 |
| Institute of Gender Health | 46.6 |
| Institute of Genetics | 37.7 |
| Institute of Cancer Research | 6.3 |
| Institute of Aging | 4.7 |
Figure 13: Rough Percentages of Citations of CIHR-Supported Cardiovascular Related Research by Continent (2008/09-2014/15)
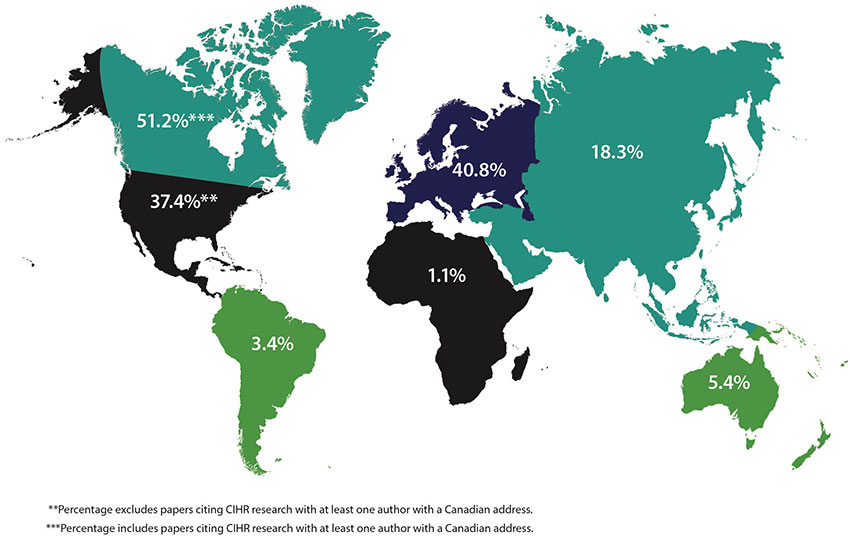
Figure 13 long description
| Continent | Rough Percentages of Citations of CIHR-Supported Cardiovascular Related Research by Continent (2008/09-2014/15) |
|---|---|
| Canada | 51.2%Footnote *** |
| Europe | 40.8% |
| United States & Central America | 37.4%Footnote ** |
| Asia | 18.3% |
| Australia | 5.4% |
| South America | 3.4% |
| Africa | 1.1% |
|
|
Answering the remaining complex questions needed for the continued and advanced diagnosis, treatment, management and cure of circulatory and respiratory diseases requires ICRH to work with its peer Institutes to bring together the needed Canadian expertise. ICRH is a proponent of collaboration as a means to success and is committed to contributing to the overlapping objectives of other Institutes. The Institute will continue to develop opportunities for researchers in large scale multi-Institute initiatives where increased networking will be the norm. Valuing the sharing of Canadian knowledge and export that comes with increased scientific collaboration, ICRH will take advantage of available opportunities to position our research community poised to join in national and international collaboration.
Building Canadian Expertise
CANUE a National Network
The Canadian Urban Environmental Health Research Consortium (CANUE) is a national, open-membership consortium with multi-disciplinary representation from the fields of environmental health research, health policy, and urban design and planning. Funded as part of the CIHR Roadmap Accelerator Fund, CANUE is focused on developing big-data tools to examine the interaction between the physical features of the urban environment and health. Findings from CANUE are expected to lead to cost-effective actions that promote healthy childhood development and aging, reduce the burden of chronic disease and minimize the impact of changing environments. As a key contributor, the ICRH recognizes the role national cohorts like CANUE play in generating Canadian capacity and building internationally recognized research expertise.
International Collaboration
The Global Alliance on Chronic Disease
With scientific expertise in each of the Institute mandate areas, ICRH is committed to promoting platforms that facilitate international collaboration for Canadian researchers. In collaboration with two other CIHR Institutes, ICRH has funded two Team Grants as part of the Global Alliance on Chronic Disease: Prevention of Chronic Lung Disease initiative. The RETRAC2 study focuses on developing community commercial tobacco reduction strategies in Canada’s Indigenous communities, while the Examining the impact of tobacco pricing and packaging strategies on tobacco use and equity in middle-income countries is a collaboration of Canadian, Chilean, Columbian, South African, Vietnamese and Ecuadorian researchers studying the impact of tobacco prices on smoking practices and consumption. ICRH understands the significance of these collaborative opportunities for Canadian researchers and when possible will continue the support international research initiatives.
Objective #4
Research has led to a dramatic improvement in survival from catastrophic events such as heart attack and stroke, and improved the wellbeing of persons suffering from chronic circulatory and respiratory disease. For example, since 1970 the death rate from cardiovascular disease has fallen nearly five-fold from roughly 500 to 100 per 100,000 population by 2010Footnote 8. In the face of this incredible advance, however, the benefit has not distributed equally across populations. Both women (and those identifying with the female gender) and Indigenous persons experience relatively poorer outcomes from circulatory and respiratory events than their age-matched counterparts. Such inequity in patient outcomes is inexcusable and ICRH and its community of researchers are poised to address these disparities.
Equity is an integral part of a sustainable research ecosystem. Beyond the fact that all researchers should have equal and fair access to funding for their research, equity also allows for diversity in the system, which leads to more creative, innovative, and meaningful outcomes.
The Government of Canada and CIHR have major activities underway to address inequities that exist for Indigenous persons and among genders. These are elaborated upon within two plans: the Action Plan: Building a healthier future for First Nations, Inuit and Métis PeoplesFootnote 9 and the Strategic Action Plan on Equity. Footnote 10
In November 2016, CIHR announced its action plan for building a healthier future for First Nations, Inuit and Métis Peoples in which it commits to ten actions, including the increase of investments in Indigenous Health Research (IHR) to a minimum of 4.6% (proportional to Canada’s Indigenous population) of CIHR’s annual budget. The actions were tabled in spring 2015, by the Aboriginal Health Research Steering Committee, and identify concrete steps by which CIHR can make a meaningful contribution to the wellbeing of Canada’s Indigenous Peoples through IHR.
Building a Strong Foundation
Network Environments for Indigenous Health Research
Recognizing the significance of the CIHR strategic research priority area of Health and Wellness for Indigenous Peoples, ICRH has committed to the role of co-lead with the Institute of Indigenous Peoples' Health for the upcoming Network Environments for Indigenous Health Research (NEIHR) initiative. The NEIHR is a multi-year, multi-million dollar research initiative focused on establishing a solid foundation for Indigenous health research driven by and grounded in Indigenous communities in Canada. The NEIHR is dedicated to developing an enduring Indigenous research environment network with a sustainable mandate to build research capacity, conduct research, advance Indigenous research paradigms and carry out KT.
Figure 14: CIHR’s Action Plan on Equity
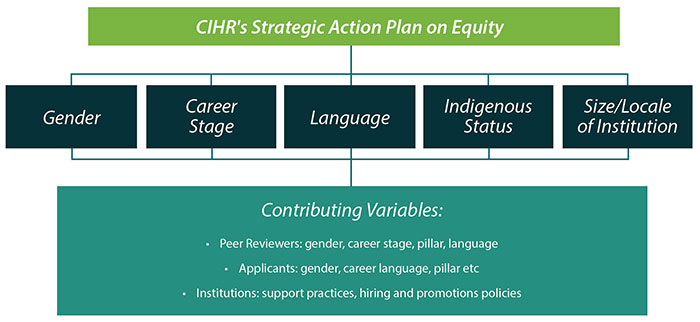
Figure 14 long description
CIHR’s Action Plan on Equity:
- Gender
- Career Stage
- Language
- Indigenous Status
- Size/Locale of Institution
Contributing Variables:
- Peer Reviewers: gender, career stage, pillar, language
- Applicants: gender, career, language, pillar, etc.
- Institutions: support practices, hiring and promotions policies
The vision of CIHR’s Strategic Action Plan on Equity is two-fold:
- To create an equitable funding system by identifying and eliminating biases towards any individual or group that would hinder access to CIHR funds; and
- To influence the larger health research community to adopt more equitable practices.
The Action Plan supports CIHR’s input to the federal government’s Gender Based Analysis Plus FrameworkFootnote 11 which requires all federal programs to consider the potential impacts of policies, programs, services, and other initiatives on diverse groups of women and men, taking into account gender and other identity factors.
The "plus" in the name highlights that the framework directs that government policy and programming look beyond gender, to include the examination of a range of other intersecting identity factors (such as: age, education, language, geography, culture and income).
Within these two frameworks, ICRH will work to support both impactful science and an equitable funding system in its mandate areas. It commits to work with colleagues, partners and communities to increase support for IHR: being research in any field or discipline related to health and/or wellness that is conducted by, grounded in, or engaged with, Indigenous communities, societies or individuals and their wisdom, cultures, experiences or knowledge systems, as expressed in their dynamic forms, past and present. IHR embraces the intellectual, physical, emotional and/or spiritual dimensions of knowledge in creative and interconnected relationships with peoples, places and the natural environment. Such research is based on the right to respectful engagement and equitable opportunities; it honours culture, language, history and traditions. Whatever the methodologies or perspectives that apply in a given context, researchers who conduct Indigenous research, whether they are Indigenous or non-Indigenous themselves, commit to respectful relationships with Indigenous Peoples and communities. It also commits to contributing to improved equity for populations known to be experiencing sub-optimal outcomes and for whom action can be taken.
About CIHR
CIHR’s mandate is to excel, according to internationally accepted standards of scientific excellence, in the creation of new knowledge and its translation into improved health for Canadians, more effective health services and products and a strengthened Canadian healthcare system.
A unique and interdisciplinary feature of CIHR is the 13 Institutes which enable CIHR to support and integrate a broad spectrum of research across the mandate areas of the Institutes. Within their mandate areas, the Institutes bring together researchers, health professionals and policy-makers from voluntary health organizations, provincial government agencies, international research organizations and industry and patient groups from across the country to create a research agenda to improve the health for Canadians, and address health research gap areas.
CIHR integrates research through a unique interdisciplinary structure made up of 13 "virtual" Institutes. The Institutes are not buildings or research centres, but networks of researchers brought together to focus on important health problems. Unconstrained by bricks and mortar, the Institutes' virtual structure encourages partnership and collaboration across sectors, disciplines and regions.
CIHR's 13 Institutes share responsibility for achieving the fundamental objective of CIHR by developing strategic priorities that are aligned with the overarching directions, mandate and vision of CIHR. The Institutes promote and build upon Canada's firm foundation of research excellence, engage the research community and encourage interdisciplinary, integrative health research.
The health research landscape has changed markedly since CIHR was created in 2000. The speed of discovery, convergence of disparate research fields and evolving health needs of Canadians are creating a number of significant, mutually reinforcing trends that are changing the way health research and knowledge translation are being conducted.
CIHR’s Strategic Plan, Health Research Roadmap II: Capturing innovation for better health and healthcare (Roadmap II) was designed to provide strategic attention to important areas identified by the research and stakeholder communities including:
- Enhanced patient experiences and outcomes through health innovations;
- Health and wellness for Indigenous Peoples;
- A healthier future through preventive action;
- Improved quality of life for persons living with chronic disease.
Today’s health challenges are increasingly complex, and finding new, innovative solutions requires partnership and collaboration across the entire health spectrum. Delivering on a national health research agenda will require contributions from all members of the Canadian health research enterprise.
CIHR continues to evolve to keep pace with the reality faced by researchers. The Institutes remain centrally important to CIHR, and a series of ongoing enhancements are being implemented to better support them and CIHR’s overall operational effectiveness. The goal is to ensure that investments in health research have the greatest possible impact on the health and wellness of Canadians.
About The ICRH Strategic Planning Process
Past-President Dr. Alain Beaudet, along with his senior executive, oversaw the launch of several initiatives designed to position CIHR as ready to respond to the changing environment in which health researchers operate. These included the release of the Strategy for Patient-Oriented Research (SPOR), a collective national effort to place patient views and perspectives at the heart of research activities, engage patients as partners, focus on patient-identified priorities and improves patient outcomesFootnote 13. Reforms to the manner in which federal granting is conducted have been progressing, with an eye towards improving efficient, equitable and transparent release of funds under an increasingly competitive granting environment.
It also saw the first Federal change in government in more than a decade, which brought forward new priorities and directions for research investment from Canadian citizens, including the Fundamental Science Review in 2017. The Government of Canada's response to the Fundamental Science Review’s Report Investing in Canada’s Future: Strengthening the Foundations of Canadian ResearchFootnote 14 will shape the way in which the research community comes together to address the complex health care challenges of the future over the next few years. For example, the Minister of Science recently announced the appointment of the first Chief Science Advisor (Dr. Mona Nemer) and the formation of the Canada Research Coordinating Committee. Correspondingly, ICRH will respond as new opportunities arise for its research community to make its contribution.
Because of continued uncertainty for the research community, ICRH decided not to develop a de novo long term strategic plan in its first years of operation. Rather ICRH worked with its community leaders to refresh its priorities and identify objectives to be reached in a shorter period. It also worked to gather information directly from the research community that identifies with the ICRH mandate, either self-identified or identified directly through receipt of ICRH funding.
Consultations with ICRH stakeholders took three forms: the formation of a temporary Strategic Planning Advisory Committee whose membership included research leadership from across its community of stakeholders (See details in Annex 1), a survey of researchers and direct engagement of ICRH’s main funding recipients.
Strategic Planning Advisory Committee (SPAC)
ICRH struck a Strategic Planning Advisory Committee (for membership see Annex 1) in order to see the community’s needs accurately reflected in the ongoing work to re-visit the Institute's priorities so as to address the changing research landscape. Its members were drawn from past ICRH Institute Advisory Board members, researchers with knowledge of the breadth of ICRH’s mandate areas, researchers at the start of their independent careers, and partners from the industry and charitable sectors. The Committee met four times over the course of a twelve month period to provide ICRH staff with inputs and reflections on concepts being developed and information being collected regarding the potential activities which could be enacted to further the mission of ICRH. Members also acted as bi-directional conduits of knowledge between ICRH and the research community during this process.
Survey
The ICRH team prepared a survey of its community to gather inputs on three important aspects of its activities: researchers’ perspective on the ICRH mandate reflecting their principal work, whether the past strategic priorities were still relevant and what aspects of training and career development were seen as most valuable. The survey, which was promoted through ICRH’s communications avenues, was open March through May 2017 and gathered 97 responses.
Funding Recipient Consultations
Perhaps more so than any other of CIHR’s Institutes, ICRH has focused, over the past strategic planning cycle, on coalescing researchers across its mandate areas into large teams and networks. Through four separate calls for requests for application launched between 2013 and 2015, ICRH funded three Emerging Networks (one call) and five teams under the Community Development Program (three calls). These are:
- Emerging Networks (funding October 2013–2018):
- The Canadian Stroke Prevention Intervention Network (C-SPIN);
- The Canadian Vascular Network (CVN); and
- The Canadian Respiratory Research Network (CRRN).
- Community Development Program Teams (funding September 2014–2019):
- The Canadian Stroke Trials for Optimized Results (CaSTOR); and
- The Canadian Critical Care Trials Group (CCCTG).
- Community Development Program Teams (funding October 2015–2020):
- The Canadian Venous Thromboembolism Clinical Trials and Outcomes Research Network (CanVECTOR);
- The Canadian Resuscitation Outcomes Consortium (CanROC); and
- The Canadian Sleep and Circadian Network (CSCN).
The Emerging Networks and Community Development Program teams differ principally on the scale of their breadth and scope, in terms of their existing size and connectivity and available existing or accessible partner resources. ICRH tasked these research consortia to fulfill, within their potential, multiple strategic priorities which it had identified as important in its plan for 2013/14–2016/17. These include:
- Identifying key knowledge gaps and promoting national & international collaborations to address those gaps;
- Building a critical mass of technical and scientific expertise on a national scale to promote the sharing of ideas, tools, methods and scarce resources;
- Actively engaging patient representatives in research planning & decision making;
- Incorporating significant training, mentoring and career development mandates within their research programs;
- Accelerating the translation of biomedical discoveries into clinical applications and best practice and marketplace;
- Integrate research & knowledge translation projects into coherent programs to generate solutions with an aim to developing, validating and implementing interventions that change a significant aspect of practice; and
- Evaluating outcomes to demonstrate impact and added-value within respected field.
These research consortia are reaching milestones on different timeframes with respect to their activity reports. In addition to reviewing formal reports and external advice on those reports, ICRH took specific action to gather insights on their progress, challenges and plans on sustainability in the process of reflecting on the past strategic priorities. It is apparent that the consortia strategy is demonstrating value by mobilizing national leaders, researchers, and partners to solve complex research questions and support the development of a strong pipeline of new, diverse and skilled researchers across all themes. However; these investments place an additional challenge to providing a comprehensive program of supports to our research community until these funding commitments end, their full impact is evaluated and their contribution to reaching past objectives discerned.
Annex 1: ICRH Strategic Planning Advisory Committee
Liam Brunham
Assistant Professor
Department of Medicine
University of British Columbia
Elaine Chong
Director
Pharmaceutical Services
British Columbia Ministry of Health
Shurjeel Choudhri (Co-Chair)
Senior Vice President and Head
Medical and Scientific Affairs, Bayer Inc.
Deborah Cook
Professor
Department of Medicine
McMaster University
John Fleetham
Professor
Department of Medicine
University of British Columbia
Malcolm King
Scientific Director
Saskatchewan Centre for Patient-Oriented Research
University Saskatchewan
Melissa Parker
Associate Professor
Department of Pediatrics
McMaster University
Andrew Pipe
Professor
Department of Medicine
University of Ottawa
Brian H. Rowe (Co-Chair)
Scientific Director
Institute of Circulatory and Respiratory Health
Michael Schull
Professor
Department of Medicine
University of Toronto
Alex Thiel
Professor
Department of Neurology & Neurosurgery
McGill University
Phil Wells
Professor (Chair and Chief)
Department of Medicine
University of Ottawa
Lori West
Professor
Department of Medicine
University of Alberta
Terms of Reference
Authority: Canadian Institutes of Health Research (CIHR)
Accountability: Institute of Circulatory and Respiratory Health (ICRH)
Chairs and Membership: The ICRH Strategic Planning Advisory Committee will be Co-Chaired by the Scientific Director of ICRH and a member of a body established by CIHR to provide direction to the organization as a whole (e.g. Governing Council, Science Council, Institute Advisory Boards, and/or their sub-committees). It will consist of members who are knowledgeable stakeholders in circulatory and respiratory research and its application in advancing the health of Canadians, who are able to contribute to the refresh of ICRH’s strategic plan for implementation over the next two years.
The Committee will be composed of no more than 14 members invited as follows:
- 1 or more representatives from CIHR’s Governing Council, Science Council and/or Institute Advisory Boards, or their sub-committees, one of whom will serve as co-Chair,
- the Scientific Director of ICRH,
- 6 to 8 representatives whose experience best fulfills a matrix covering:
- research areas within ICRH’s mandate (circulatory, respiratory, stroke, sleep, vascular and urgent care);
- CIHR’s strategic research priorities (health innovation, chronic disease, Indigenous Peoples’ health, prevention); and
- representatives from across the research pillars (biomedical, clinical, health services and social, cultural, environmental and population health) and public and private sectors (federal, provincial/territorial, industry, academic, non-governmental organizations) funders, educators etc.
- 1 or more early career investigator representatives
Terms: Members are asked to serve for an expected term of 12 months with the possibility of extension.
Meetings: Meetings will be held at the call of the Co-Chairs. Meetings will be either face-to-face, virtual or by teleconference, with the majority of the Committee’s work conducted at a distance. Secretariat support will be provided by ICRH.
Quorum: A majority of its members (50% plus 1).
Decision Making: The ICRH Strategic Planning Advisory Committee is advisory and will make decisions by consensus.
Mandate: The Committee will assist in the refreshing of ICRH’s Strategic Plan, which will provide direction to the Institute as it works to advance its mandate over a three year period between 2017/18 and 2019/20 and expand its impact, and that of CIHR, through both funded and unfunded activities. Such activities include but are not limited to: the launch and execution of funding opportunities, development and nurturing of novel partnerships, identification of opportunities for innovative collaborations and promotion of research in advancing the health of Canadians by:
- Providing input and advice on additional reference materials which should be considered in the context of other documents identified by CIHR and ICRH as important to the strategic planning process;
- Providing input and advice on the development of a series of consultations to be held with stakeholders, including the development of agendas, consultation documents, and identification of key speakers and participants;
- Attending one or more consultations and leading discussions;
- Reviewing and providing feedback and advice with respect to analysis and summaries of the discussions developed from consultations;
- Reviewing and providing feedback and advice with respect to the draft document encompassing the ICRH Strategic Plan; and
- Providing awareness of issues to be addressed in and support the dissemination and promotion of the ICRH Strategic Plan among their respective communities of stakeholders vested in ICRH.
Compensation: Service on the Committee is voluntary. Members will be reimbursed for expenses incurred to attend face-to-face meetings. While they will not receive honoraria or other financial compensation, members' contributions will be acknowledged in the final ICRH Strategic Plan 2017/18–2019/20.
Appointments: Appointments to the Committee will be made by the Scientific Director of ICRH.
*Terms of Reference were informed by Stanford, Gregory. (1995). "Bourinot’s Rules of Order”.
- Date modified: